Lumbosacral Plexus MRI Protocol and planning
Indications for lumbosacral plexus MRI scan
- Malignancy or peripheral nerve masses
- For radiation and surgical treatment planning
- Unexplained plexopathy
- Lumbosacral plexus tumors
- Sacral or coccyx pain
- Leg pain or sciatica
- Trauma
lumbosacral plexus anatomy
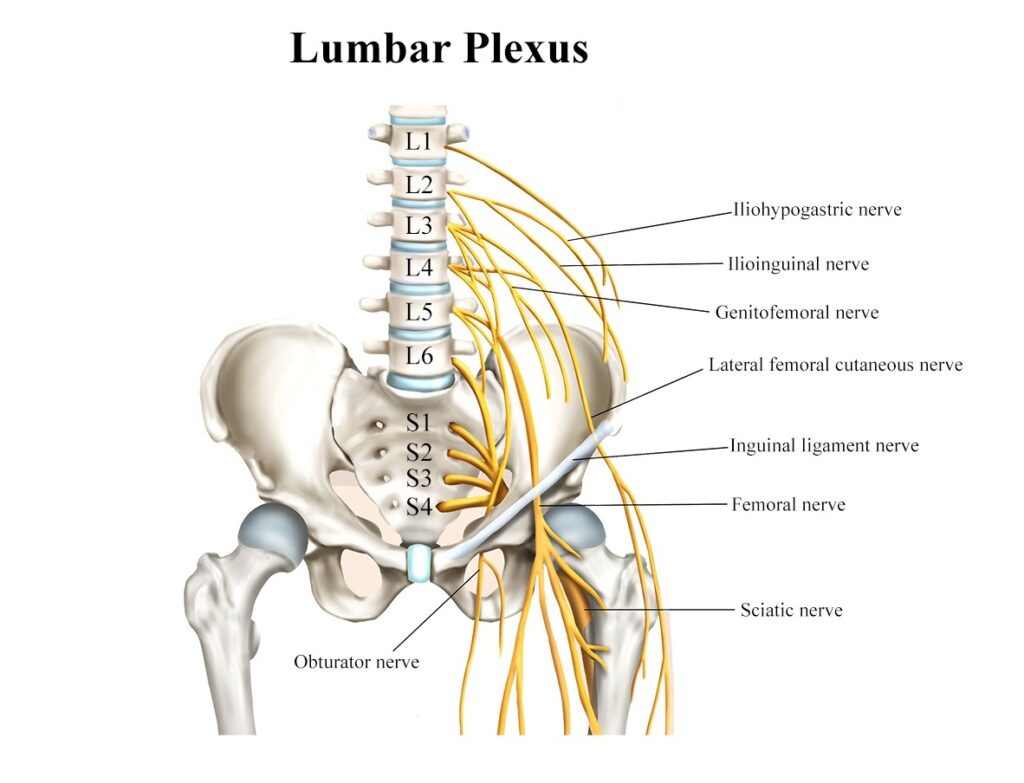
The lumbosacral plexus is a complex network of nerves that arises from the lumbar and sacral spinal nerves (L1 to S4) and supplies the lower extremities, pelvis, and some parts of the abdominal wall. It is formed by the intertwining and branching of multiple nerves, and its main function is to provide motor and sensory innervation to the lower limbs and pelvis. Here’s an overview of the major nerves and components of the lumbosacral plexus:
- Lumbar Plexus (L1-L4): The lumbar plexus is the upper portion of the lumbosacral plexus and is formed by the ventral rami of the first four lumbar nerves (L1 to L4). It lies within the psoas major muscle and gives rise to several important nerves, including:
- Iliohypogastric nerve (L1): Provides motor innervation to the transversus abdominis and internal oblique muscles, and sensory innervation to the skin of the lower abdomen.
- Ilioinguinal nerve (L1): Supplies the skin of the upper medial thigh, the mons pubis, and the labia majora in females or the root of the penis and scrotum in males.
- Genitofemoral nerve (L1-L2): Divides into two branches – the genital branch, which supplies the cremaster muscle in males and sensory innervation to the scrotum or labia majora, and the femoral branch, which provides sensory innervation to the skin of the upper anterior thigh.
- Lateral femoral cutaneous nerve (L2-L3): Supplies sensory innervation to the lateral thigh.
- Femoral nerve (L2-L4): The largest nerve of the lumbar plexus, it provides motor innervation to the quadriceps femoris muscle group, sartorius, and iliacus muscles, and sensory innervation to the anterior thigh and medial leg and foot.
- Sacral Plexus (L4-S4): The sacral plexus is the lower portion of the lumbosacral plexus and is formed by the ventral rami of the last lumbar nerve (L4) and the sacral nerves (S1 to S4). It lies on the posterior aspect of the pelvis and gives rise to the following major nerves:
- Superior gluteal nerve (L4-S1): Supplies the gluteus medius, gluteus minimus, and tensor fasciae latae muscles, which are responsible for hip abduction and medial rotation.
- Inferior gluteal nerve (L5-S2): Innervates the gluteus maximus muscle, responsible for hip extension and lateral rotation.
- Sciatic nerve (L4-S3): The largest nerve in the body, it is formed by the fusion of the ventral rami of L4 to S3. The sciatic nerve runs down the posterior thigh and divides into two terminal branches – the tibial nerve and the common fibular (peroneal) nerve.
- Tibial nerve (L4-S3): Supplies the posterior thigh muscles and almost all the muscles in the leg and foot, controlling ankle plantar flexion and foot inversion.
- Common fibular (peroneal) nerve (L4-S2): Divides into the superficial fibular nerve and the deep fibular nerve. It controls dorsiflexion of the foot and the muscles of the anterior and lateral leg.
Contraindications
- Any electrically, magnetically or mechanically activated implant (e.g. cardiac pacemaker, insulin pump biostimulator, neurostimulator, cochlear implant, and hearing aids)
- Intracranial aneurysm clips (unless made of titanium)
- Pregnancy (risk vs benefit ratio to be assessed)
- Ferromagnetic surgical clips or staples
- Metallic foreign body in the eye
- Metal shrapnel or bullet
Patient preparation for lumbosacral plexus MRI scan
- A satisfactory written consent form must be taken from the patient before entering the scanner room
- Ask the patient to remove all metal object including keys, coins, wallet, any cards with magnetic strips, jewellery, hearing aid and hairpins
- Ask the patient to undress and change into a hospital gown
- Contrast injection risk and benefits must be explained to the patient before the scan
- Gadolinium should only be given to the patient if GFR is > 30
- If possible, provide a chaperone for claustrophobic patients (e.g. relative or staff )
- Offer earplugs or headphones, possibly with music for extra comfort
- Explain the procedure to the patient
- Instruct the patient to keep still
- Note the weight of the patient
Positioning for lumbosacral plexus MRI
- Position the patient in supine position with head pointing towards the magnet (head first supine)
- Position the patient over the spine coil and place the body coils over the pelvis and abdomen (nipple down to three inches below symphysis pubis)
- Securely tighten the body coil using straps to prevent respiratory artefacts
- Give a pillow under the head and cushions under the legs for extra comfort
- Centre the laser beam localiser over the iliac crest
Recommended Lumbosacral Plexus MRI Protocols and Planning
Lumbosacral Plexus MRI Localizer

A three-plane localizer must be taken at the beginning to localize and plan the sequences. Localizers are normally less than 25 seconds and are T1\T2-weighted low-resolution scans.

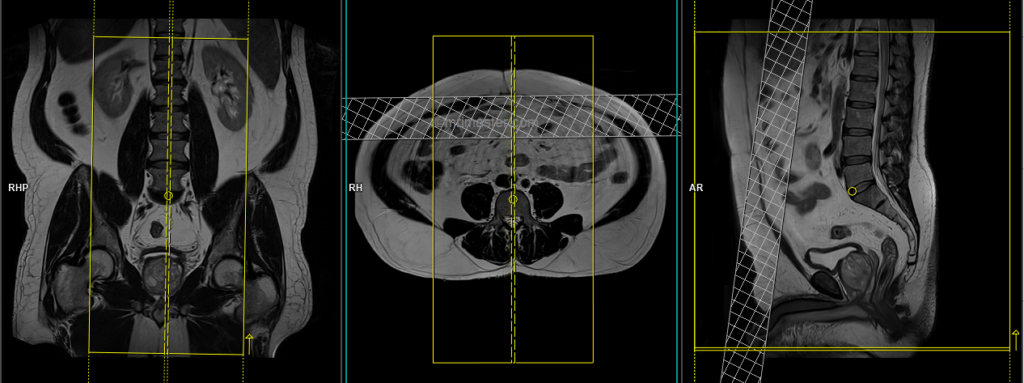
T2 tse sagittal 3mm
Plan the sagittal slices on the coronal plane and angle the planning block parallel to the spinal cord. Check the positioning block in the other two planes, ensuring an appropriate angle is given in the axial plane (parallel to the center of the vertebral body and the spinous process). Verify the position block in the sagittal plane; the field of view (FOV) must be big enough to cover the entire lumbosacral plexus from L1 down to the pubic symphysis (normally 350mm). Ensure that the slices are sufficient to cover the nerves from the right acetabulum to the left acetabulum. The phase direction should be head to feet to avoid motion artifacts from the abdomen.
Parameters
TR 4000-5000 | TE 100-120 | SLICE 3 MM | FLIP 130-150 | PHASE H>F | MATRIX 448X384 | FOV 350-350 | GAP 10% | NEX(AVRAGE) 2 |
T1 tse coronal 3mm
Plan the coronal slices on the sagittal plane; angle the planning block parallel to the spinal canal. Check the positioning block in the other two planes. An appropriate angle must be given in the axial plane (parallel to the right and left psoas muscle). Check the positioning block in the sagittal plane; FOV must be big enough to cover the whole lumbosacral plexus from L1 down to the pubic symphysis (normally 350mm). Slices must be sufficient to cover the nerves from the anterior border of the symphysis pubis to the median sacral crest. Adding a saturation band in front of the coronal block will reduce artifacts from breathing and peristalsis.

Parameters
TR 400-600 | TE 15-25 | SLICE 3 MM | FLIP 150 | PHASE R>L | MATRIX 512X380 | FOV 350-350 | GAP 10% | NEX(AVRAGE) 2 |
T2 STIR coronal 3mm
Plan the coronal slices on the sagittal plane; angle the planning block parallel to the spinal canal. Check the positioning block in the other two planes. An appropriate angle must be given in the axial plane (parallel to the right and left psoas muscle). Check the positioning block in the sagittal plane; FOV must be big enough to cover the whole lumbosacral plexus from L1 down to the pubic symphysis (normally 350mm). Slices must be sufficient to cover the nerves from the anterior border of the symphysis pubis to the median sacral crest. Adding a saturation band in front of the coronal block will reduce artifacts from breathing and peristalsis.
Parameters
TR 4000-5000 | TE 110 | FLIP 160 | NEX 2 | SLICE 3 MM | MATRIX 384X320 | FOV 350-350 | PHASE R>L | GAP 10% | TI 150 |
T2 space 3D 1mm isotropic coronal
Plan the coronal 3D block on the sagittal plane; angle the planning block parallel to the spinal canal. Check the positioning block in the other two planes. An appropriate angle must be given in the axial plane (parallel to the right and left psoas muscle). Check the positioning block in the sagittal plane; FOV must be big enough to cover the whole lumbosacral plexus from L1 down to the pubic symphysis (normally 350mm). Slices must be sufficient to cover the nerves from the anterior border of the symphysis pubis to the median sacral crest. Adding a saturation band in front of the coronal block will reduce artifacts from breathing and peristalsis.

Parameters
TR 2000-3000 | TE 90-100 | SLICE 1MM | FLIP 160-170 | PHASE R>L | MATRIX 384X320 | FOV 330-350 | GAP 10% | NEX(AVRAGE) 2 |
T1 TSE Axial 3mm SFOV
Plan the axial slices on the sagittal plane; angle the planning block perpendicular to the spinal canal. Check the positioning block in the other two planes. An appropriate angle must be given in the coronal plane (perpendicular to the lumbar spines). Slices must be sufficient to cover the lumbosacral plexus from L1 down to the pubic symphysis.

Parameters
TR 400-600 | TE 15-25 | SLICE 3 MM | FLIP 150 | PHASE R>L | MATRIX 384X320 | 250-300 | GAP 10% | NEX(AVRAGE) 2 |
T2 stir Axial 3mm SFOV
Plan the axial slices on the sagittal plane; angle the planning block perpendicular to the spinal canal. Check the positioning block in the other two planes. An appropriate angle must be given in the coronal plane (perpendicular to the lumbar spines). Slices must be sufficient to cover the lumbosacral plexus from L1 down to the pubic symphysis.
Parameters
TR 4000-5000 | TE 110 | FLIP 150 | NEX 2 | SLICE 3 MM | MATRIX 320X320 | FOV 250-300 | PHASE R>L | GAP 10% | TI 150 |
Contrast enhanced lumbosacral plexus
Use T1 TSE Fat saturated axial and coronal scans after the administration of IV gadolinium DTPA injection(copy the planning outlined above). The document below provides access to the recommended dosage of gadolinium DTPA injection, as advised by the manufacturer.
Optional Scans
T1 VIBE DIXON 3D 1mm isotropic coronal post contrast
Plan the coronal 3D block on the sagittal plane; angle the planning block parallel to the spinal canal. Check the positioning block in the other two planes. An appropriate angle must be given in the axial plane (parallel to the right and left hip joint). Check the positioning block in the sagittal plane; FOV must be big enough to cover the whole lumbosacral plexus from L1 down to the pubic symphysis (normally 350mm). Slices must be sufficient to cover the nerves from the anterior border of the symphysis pubis to the median sacral crest. Adding a saturation band in front of the coronal block will reduce artifacts from breathing and peristalsis.
Parameters
TR 6-7 | TE 2.39 4.77 | SLICE 1 MM | FLIP 12 | PHASE A>P | MATRIX 384X384 | FOV 330-350 | GAP 10% | NEX(AVRAGE) 2 |