Psoas Muscle MRI Protocols and planning
Indications of psoas muscle MRI scan
- Tuberculosis of spine
- Iliopsoas tendon rupture
- Iliopsoas syndrome
- Iliopsoas cyst
- Psoas abscess
Psoas muscle Anatomy
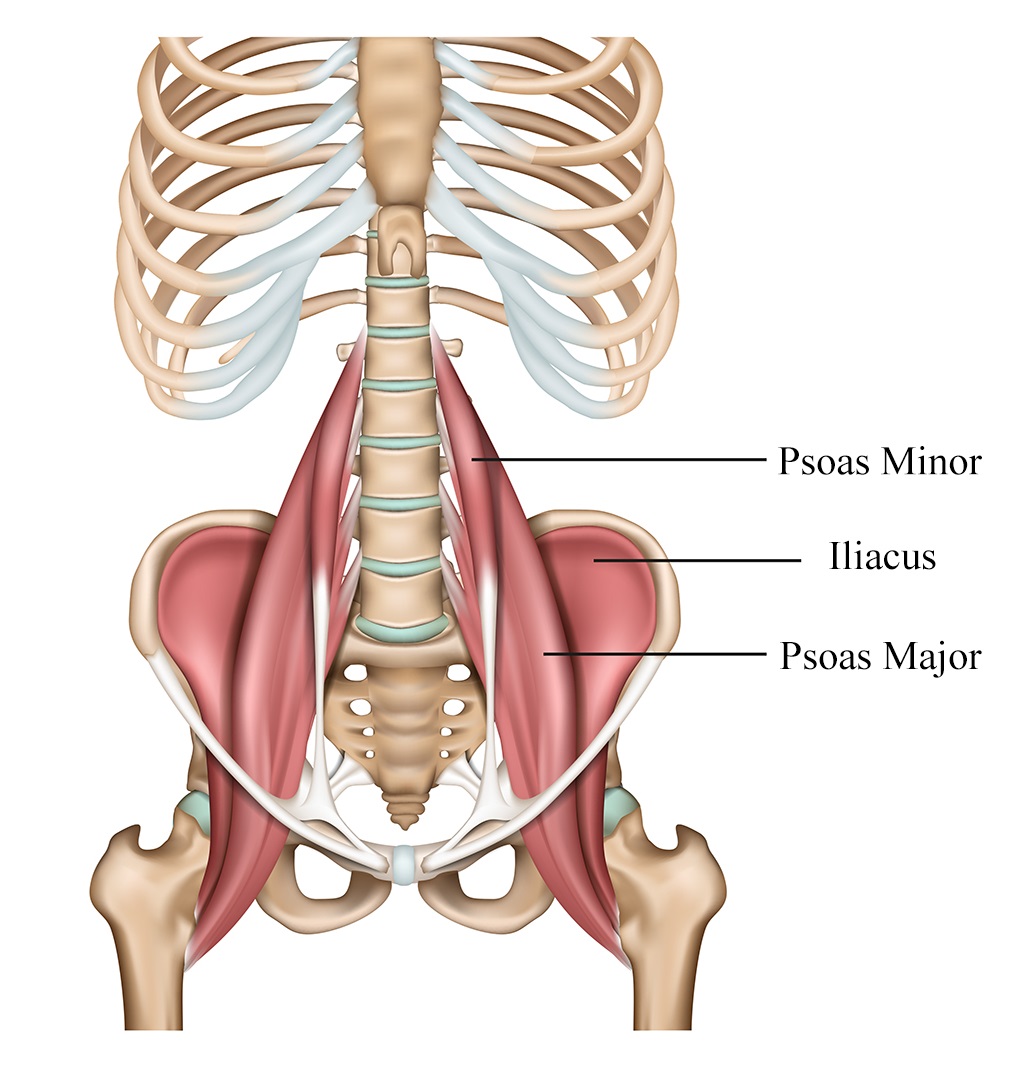
The psoas muscle, also known as the iliopsoas, is a large and powerful muscle located deep within the abdomen and pelvis. It is actually made up of two muscles: the psoas major and the iliacus, which work together as a single functional unit. The psoas muscle plays a crucial role in hip flexion, stability of the lumbar spine, and overall posture.
Anatomy:
Psoas Major: The psoas major originates from the lumbar vertebrae (specifically T12 to L5) of the lower spine. It travels downward and laterally, passing through the pelvic region, and inserts onto the lesser trochanter of the femur, which is a bony prominence on the inner side of the thigh bone (femur).
Iliacus: The iliacus muscle arises from the iliac fossa, which is part of the iliac bone of the pelvis. It also travels downward and laterally to join the psoas major at the same insertion point on the lesser trochanter of the femur.
Function: The primary function of the psoas muscle is hip flexion, which involves bringing the thigh towards the abdomen. This action is crucial for activities like walking, running, climbing stairs, and lifting the legs while lying down. Additionally, the psoas muscle helps stabilize the lumbar spine during these movements, providing support and preventing excessive arching of the lower back.
The psoas muscle is often involved in activities that require core stabilization, such as maintaining balance and performing various movements that engage the abdominal muscles. Because of its deep location within the body, the psoas muscle is considered a key player in maintaining proper posture and stability during both static and dynamic activities.
Clinical Significance: Due to its deep location and close proximity to vital structures, the psoas muscle can be a source of pain and discomfort. Psoas muscle strain or irritation can occur due to overuse, improper technique during physical activities, or prolonged sitting. When inflamed or irritated, the psoas muscle can cause pain in the lower back, groin, and hip regions.
Psoas muscle 3d image
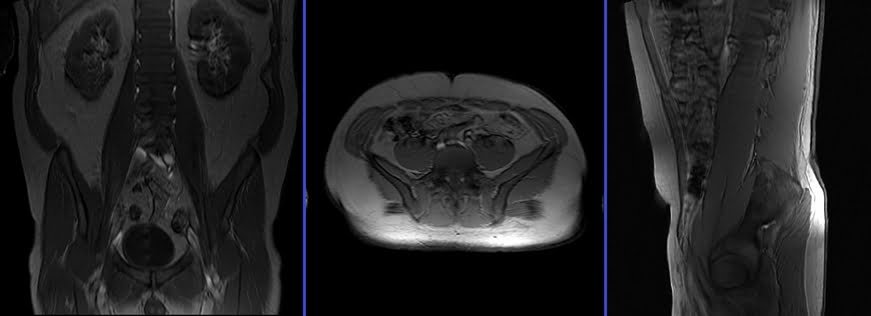
psoas muscle mri image

Contraindications
- Any electrically, magnetically or mechanically activated implant (e.g. cardiac pacemaker, insulin pump biostimulator, neurostimulator, cochlear implant, and hearing aids)
- Intracranial aneurysm clips (unless made of titanium)
- Pregnancy (risk vs benefit ratio to be assessed)
- Ferromagnetic surgical clips or staples
- Metallic foreign body in the eye
- Metal shrapnel or bullet
Patient preparation for psoas muscle MRI
- A satisfactory written consent form must be taken from the patient before entering the scanner room
- Ask the patient to remove all metal object including keys, coins, wallet, any cards with magnetic strips, jewellery, hearing aid and hairpins
- Ask the patient to undress and change into a hospital gown
- If possible provide a chaperone for claustrophobic patients (e.g. relative or staff )
- Offer earplugs or headphones, possibly with music for extra comfort
- Explain the procedure to the patient
- Instruct the patient to keep still
- Note the weight of the patient
Positioning for psoas muscle MRI
- Position the patient in supine position with head pointing towards the magnet (head first supine)
- Position the patient over the spine coil and place the body coils over abdomen and pelvis (nipple down to elbow three inches below symphysis pubis)
- Securely tighten the body coil using straps to prevent respiratory artefacts
- Give a pillow under the head and cushions under the legs for extra comfort
- Centre the laser beam localiser over the iliac crest
- Register the patient in the scanner as head first supine

Recommended Psoas Muscle MRI Protocols and Planning
Psoas muscle MRI localiser
A three-plane localizer must be taken at the beginning to localize and plan the sequences. Localizers are normally less than 25 seconds and are T1\T2-weighted low-resolution scans.
T2 stir coronal 4mm large FOV
Plan the coronal slices on the sagittal plane; angle the positioning block parallel to the psoas. Check the positioning block in the other two planes. An appropriate angle must be given in the axial plane (across the right and left psoas). Slices must be sufficient to cover the whole psoas from anterior to posterior. The FOV must be big enough to cover the whole psoas (normally 400mm-450mm) from T12 down to the lesser trochanter of the femur. Adding saturation bands in front of the coronal block will reduce artifacts from arterial pulsation and breathing.

Parameters
TR 4000-5000 | TE 110 | FLIP 150 | NEX 2 | SLICE 4 MM | MATRIX 384X384 | FOV 400-450 | PHASE R>L | GAP 10% | TI 160 |
T1 tse coronal 4mm large FOV
Plan the coronal slices on the sagittal plane; angle the positioning block parallel to the psoas. Check the positioning block in the other two planes. An appropriate angle must be given in the axial plane (across the right and left psoas). Slices must be sufficient to cover the whole psoas from anterior to posterior. The FOV must be big enough to cover the whole psoas (normally 400mm-450mm) from T12 down to the lesser trochanter of the femur. Adding saturation bands in front of the coronal block will reduce artifacts from arterial pulsation and breathing.
Parameters
TR 400-600 | TE 15-25 | SLICE 4 MM | FLIP 160 | PHASE R>L | MATRIX 448X384 | FOV 400-450 | GAP 10% | NEX(AVRAGE) 2 |
T2 tse (or stir) axial 4 mm 300 fov
Plan the axial slices on the sagittal plane; angle the positioning block perpendicular to the psoas. Check the positioning block in the other two planes. An appropriate angle must be given in the coronal plane (perpendicular to the lumbar spine). Slices must be sufficient to cover the whole psoas from T12 down to the lesser trochanter of the femur. FOV must be big enough to cover the whole psoas (normally 300mm). Adding saturation bands in front of the axial block will reduce artifacts from arterial pulsation and breathing.

Parameters
TR 4000-5000 | TE 100-120 | SLICE 4 MM | FLIP 130-150 | PHASE A>P | MATRIX 320X256 | FOV 300 | GAP 10% | NEX(AVRAGE) 2 |
T1 tse axial 4 mm 300 fov
Plan the axial slices on the sagittal plane; angle the positioning block perpendicular to the psoas. Check the positioning block in the other two planes. An appropriate angle must be given in the coronal plane (perpendicular to the lumbar spine). Slices must be sufficient to cover the whole psoas from T12 down to the lesser trochanter of the femur. FOV must be big enough to cover the whole psoas (normally 300mm). Adding saturation bands in front of the axial block will reduce artifacts from arterial pulsation and breathing.
Parameters
TR 400-600 | TE 15-25 | SLICE 4 MM | FLIP 150 | PHASE A>P | MATRIX 320X320 | FOV 300 | GAP 10% | NEX(AVRAGE) 2 |