MRI of Adnexal Mass in Pregnancy
Introduction
An adnexal mass in pregnancy refers to an abnormal growth or lump found in the adnexa area, encompassing the ovaries, fallopian tubes, and surrounding tissues, during pregnancy. Although most adnexal masses detected during pregnancy are typically benign, the potential for malignancy must be considered and evaluated. Symptoms associated with adnexal masses may include pelvic pain, discomfort, or the presence of a palpable mass. Ultrasound imaging is the usual method for diagnosis, as it is the primary imaging modality employed. However, MRI scans offer additional valuable information for accurate diagnosis and management. MRI scans aid in distinguishing between benign and malignant masses, identifying complex or atypical features, and assessing the extent of tumor involvement. Detailed anatomical images provided by MRI facilitate improved characterization of the adnexal mass. Performing an MRI scan for an adnexal mass in pregnancy can be challenging due to the potential location of the lesion anywhere within the abdomen or pelvis. Radiographers must initially conduct a large field of view (FOV) abdominal and pelvic scan to locate the mass. Once the mass is identified, subsequent small FOV scans should be performed to characterize the lesion accurately.
Indications for the scan
- Adnexal mass
- ovarian cancer
- dermoid cysts
- endometriomas
- cystadenomas
- functional cysts
Contraindications
- Any electrically, magnetically or mechanically activated implant (e.g. cardiac pacemaker, insulin pump biostimulator, neurostimulator, cochlear implant, and hearing aids)
- Intracranial aneurysm clips (unless made of titanium)
- Ferromagnetic surgical clips or staples
- Metallic foreign body in the eye
- Metal shrapnel or bullet
Patient preparation
- A satisfactory written consent form must be taken from the patient before entering the scanner room
- Ask the patient to remove all metal objects including keys, coins, wallet, cards with magnetic strips, jewellery, hearing aid and hairpins
- Ask the patient to undress and change into a hospital gown
- Instruct the patient to hold their breath for the breath hold scans and breathe gently for the gated scans. It is recommended to provide coaching to the patient two to three times before initiating the scan.
- Claustrophobic patients may be accompanied into the scanner room e.g. by staff member or relative with proper safety screening
- Buscopan injection risk and benefits must be explained to the patient before the scan
- Offer headphones for communicating with the patient and ear protection
- Explain the procedure to the patient and answer questions
- Note down the hight and weight of the patient
- Pregnancy scanning consent must be taken before the procedure
Positioning
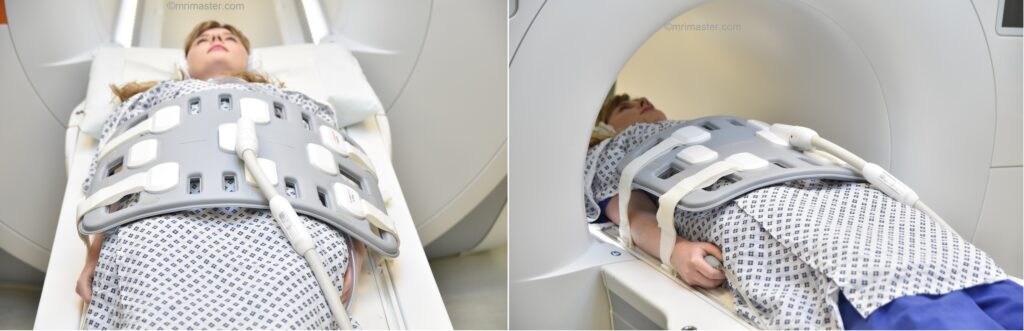
- Position the patient in supine position with head pointing towards the magnet (head first supine)
- Position the patient over the spine coil and place the body coil over abdomen and pelvis (nipple down to three inches below symphysis pubis)
- Securely tighten the body coil using straps to prevent respiratory artefacts
- Give a pillow under the head and cushions under the legs for extra comfort
- Centre the laser beam localiser over the iliac crest
- Register the patient in the scanner as head first supine
Recommended MRI Adnexal Mass in Pregnancy Protocols and Planning
localiser
To localize and plan the sequences, it is essential to acquire a three-plane T2 HASTE localizer initially. These fast single-shot localizers have an acquisition time of under 25 seconds and are highly effective in accurately localizing abdominal structures.

T2 STIR\HASTE FAT SAT 6 mm Multiple breath-hold coronal
Plan the coronal slices based on the axial image, positioning the block horizontally across the abdomen as shown below. Confirm the positioning in the other two planes. Establish an appropriate angle in the sagittal plane, aligning it vertically across the abdomen. Ensure that an adequate number of slices are acquired to cover the abdomen and pelvis, extending from the anterior abdominal wall to the spinal canal. The field of view (FOV) should be sufficiently large to encompass the abdomen and pelvis, from the xiphisternum to the pubic symphysis. To prevent wrap-around artifacts, employ phase oversampling. Instruct the patient to hold their breath during image acquisition.

Parameters
TR 2000-2500 | TE 90-110 | FLIP 130 | NEX 1 | SLICE 6MM | MATRIX 256×256 | FOV 350 | PHASE R>L | OVERSAMPLE 50% | TRIGGER NO |
T1 tse\ vibe 6 mm multiple breath-hold axial
Plan the axial slices on the coronal image by positioning the block across the abdomen as shown below. Verify the positioning in the other two planes. Establish an appropriate angle in the sagittal plane, aligning it horizontally across the abdomen. The slices must be sufficient to cover the entire lower abdomen and pelvis, ranging from the middle of the kidneys down to the symphysis pubis. Phase oversampling can be employed to prevent wrap-around artifacts. Instruct the patient to hold their breath during image acquisition.

TR 2500-3000 | TE 90-110 | FLIP 130 | NEX 1 | SLICE 5MM | MATRIX 256×256 | FOV 350 | PHASE R>L | OVERSAMPLE 50% | TRIGGER NO |
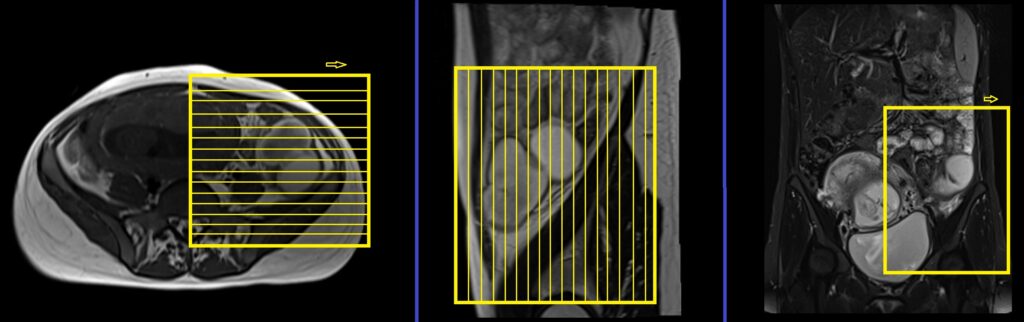
T2 TSE axial multiple breath holds 4mm SFOV
Plan the axial slices based on the coronal image, positioning the block horizontally across the adnexal mass as shown below. Verify the positioning block in the other two planes. Ensure an appropriate angle is given in the sagittal plane, perpendicular to the rectus abdominis muscle. The slices should adequately cover the adnexal mass. Select a SFOV (typically ranging from 200mm to 250mm) that sufficiently encompasses the affected area. To avoid wrap-around artifacts, consider using phase oversampling. Additionally, placing saturation bands on the top and bottom of the axial block will help reduce arterial pulsation and breathing artifacts. Instruct the patient to hold their breath during image acquisition.
This sequence is a modified version of a T2 TSE breath-hold scan commonly used in abdominal and liver imaging. To obtain high-resolution breath-hold scans, users can customize the T2 sequence. The default sequence parameters are as follows: 350-400 FOV, matrix 256×256, NEX 1, slice thickness 6mm, and acquisition of 25-30 slices within a 30-second breath hold. To achieve the desired high-resolution scan, make the following modifications: 200-250 FOV, matrix 256×192, NEX 2, and a slice thickness of 4mm with parallel imaging (IPAT) enabled. Typically, the adapted sequence will take approximately 90 seconds, requiring it to be divided into 4 acquisitions (concatenations). This division ensures that each breath-hold acquisition lasts approximately 22 seconds.

Parameters
TR 3000-4000 | TE 100 | FLIP 150 | NEX 2 | SLICE 4 MM | MATRIX 256X192 | FOV 200-250 | PHASE A>P | OVERSAMPLE 30% | IPAT On |
T1 VIBE DIXON SFOV 4mm axial breath hold
Plan the axial slices based on the coronal image, positioning the block horizontally across the adnexal mass as shown below. Verify the positioning block in the other two planes. Ensure an appropriate angle is given in the sagittal plane, perpendicular to the rectus abdominis muscle. The slices should adequately cover the adnexal mass. Select a SFOV (typically ranging from 200mm to 250mm) that sufficiently encompasses the affected area. To avoid wrap-around artifacts, consider using phase oversampling. Additionally, placing saturation bands on the top and bottom of the axial block will help reduce arterial pulsation and breathing artifacts. Instruct the patient to hold their breath during image acquisition.

Parameters
TR 7-8 | TE 2.39 4.77 | FLIP 10 | NXA 1 | SLICE 3 MM | MATRIX 224×224 | FOV 200 | PHASE R>L | OVERSAMPLE 50% | BH YES |
T2 TSE fat sat/ STIR axial multiple breath holds 4mm SFOV
Plan the axial slices based on the coronal image, positioning the block horizontally across the adnexal mass as shown below. Verify the positioning block in the other two planes. Ensure an appropriate angle is given in the sagittal plane, perpendicular to the rectus abdominis muscle. The slices should adequately cover the adnexal mass. Select a SFOV (typically ranging from 200mm to 250mm) that sufficiently encompasses the affected area. To avoid wrap-around artifacts, consider using phase oversampling. Additionally, placing saturation bands on the top and bottom of the axial block will help reduce arterial pulsation and breathing artifacts. Instruct the patient to hold their breath during image acquisition.
Parameters
TR 4000-5000 | TE 500 | FLIP 150 | NEX 1 | SLICE 4MM | MATRIX 256X208 | FOV 200-250 | PHASE R>L | OVERSAMPLE 50% | IPAT ON |
DWI epi 3 scan trace axial 4mm free breathing
Plan the axial slices based on the coronal image, positioning the block horizontally across the adnexal mass as shown below. Verify the positioning block in the other two planes. Ensure an appropriate angle is given in the sagittal plane, perpendicular to the rectus abdominis muscle. The slices should adequately cover the adnexal mass. Select a SFOV (typically ranging from 200mm to 250mm) that sufficiently encompasses the affected area. To avoid wrap-around artifacts, consider using phase oversampling. Additionally, placing saturation bands on the top and bottom of the axial block will help reduce arterial pulsation and breathing artifacts. Instruct the patient to breathe normally during image acquisition.
Parameters
TR 6000-7000 | TE 90 | IPAT ON | NEX 3 5 8 | SLICE 4 MM | MATRIX 192X192 | FOV 200-250 | PHASE R>L | GAP 10% | B VALUE 0 |
T2 TSE coronal multiple breath holds 4mm SFOV
Plan the coronal slices on the axial image and position the block horizontally across the adnexal mass as shown below. Verify the positioning block in the other two planes. Ensure an appropriate angle is given in the sagittal plane, parallel to the rectus abdominis muscle. The number of slices should be sufficient to cover the adnexal mass. Choose a SFOV (field of view) that adequately covers the affected area (typically 200mm-250mm). To prevent wrap-around artifacts, consider using phase oversampling. Additionally, placing saturation bands on the top and bottom of the axial block will help reduce arterial pulsation and breathing artifacts. Instruct the patient to hold their breath during image acquisition.
Parameters
TR 3000-4000 | TE 100 | FLIP 150 | NEX 2 | SLICE 4 MM | MATRIX 256X192 | FOV 200-250 | PHASE R>L | OVERSAMPLE 70% | IPAT On |
T2 TSE sagittal multiple breath holds 4mm SFOV
Plan the sagittal slices on the axial image and angle the positioning block approximately perpendicular to the rectus abdominis muscle. Verify the positioning block in the other two planes. Ensure an appropriate angle is set in the coronal plane, parallel to the rectus abdominis muscle. The number of slices should be adequate to encompass the adnexal mass. Select a small field of view (FOV) that adequately covers the affected area, typically ranging from 200mm to 250mm. Consider utilizing phase oversampling to prevent wrap-around artifacts. Instruct the patient to hold their breath during image acquisition.

Parameters
TR 3000-4000 | TE 100 | FLIP 150 | NEX 2 | SLICE 4 MM | MATRIX 256X192 | FOV 200-250 | PHASE A>P | OVERSAMPLE 30% | IPAT On |
Optional Scans
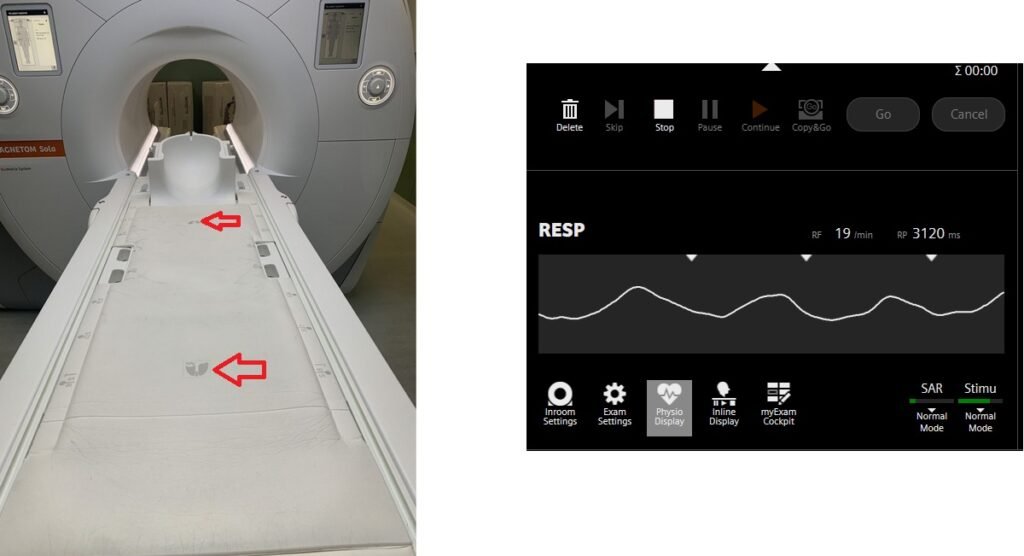
T2 HASTE axial 4 mm SFOV gated using table respiratory sensor
Respiratory gating in modern scanners can now be accomplished using built-in table respiratory sensors. This feature proves particularly beneficial when patients have irregular breathing patterns or are at risk of falling asleep during the scan. The advantage of table sensors is that they do not necessitate any specific planning. The only requirement is to ensure that the patient’s chest is accurately positioned over the table sensors to enable accurate monitoring of breathing. Additionally, it is important to select the appropriate gating option, such as the table sensor gating, in the protocol settings.
Plan the axial slices on the coronal image, positioning the block horizontally across the adnexal mass as shown below. Verify the positioning block in the other two planes. Ensure an appropriate angle is given in the sagittal plane, perpendicular to the rectus abdominis muscle. The slices should adequately cover the adnexal mass. Select a SFOV (typically ranging from 200mm to 250mm) that sufficiently encompasses the affected area. To avoid wrap-around artifacts, consider using phase oversampling. Additionally, placing saturation bands on the top and bottom of the axial block will help reduce arterial pulsation and breathing artifacts. Instruct the patient to breathe normally during image acquisition.
Parameters
TR 4000-5000 | TE 500 | FLIP 150 | NEX 1 | SLICE 4MM | MATRIX 256X224 | FOV 200-259 | PHASE R>L | OVERSAMPLE 50% | IPAT ON |
Table sensors
Advanced MRI scanners are equipped with built-in table sensors that detect the respiratory waveform and trigger data acquisition during the expiration phase of the respiratory cycle. Proper patient positioning over the sensor is critical for accurate respiratory gating. This method eliminates the need for external respiratory gating equipment, such as sensors and belts.