MRA Renal Arteries
Indications for magnetic resonance angiography (MRA) renals
- Renal vascular malformation (i.e. arteriovenous malformations and fistulae)
- For the evaluation of renal artery stenosis
- Hypertensive chronic kidney disease
- Atherosclerotic renal artery stenosis
- Fibro muscular dysplasia
- Renal artery aneurysm
- Renal artery dissection
- Renal donors
Contraindications
- Any electrically, magnetically or mechanically activated implant (e.g. cardiac pacemaker, insulin pump biostimulator, neurostimulator, cochlear implant, and hearing aids)
- Intracranial aneurysm clips (unless made of titanium)
- Pregnancy (risk vs benefit ratio to be assessed)
- Ferromagnetic surgical clips or staples
- Metallic foreign body in the eye
- Metal shrapnel or bullet
Patient preparation for MRA Renal Arteries
- A satisfactory written consent form must be taken from the patient before entering the scanner room
- Ask the patient to remove all metal objects including keys, coins, wallet, cards with magnetic strips, jewellery, hearing aid and hairpins
- Ask the patient to undress and change into a hospital gown
- Instruct the patient to hold their breath for the breath hold scans (its better to coach the patient two to three times before starting the scan)
- An intravenous line must be placed with extension tubing extending out of the magnetic bore
- Contrast injection risk and benefits must be explained to the patient before the scan
- Gadolinium should only be given to the patient if GFR is > 30
- If possible provide a chaperone for claustrophobic patients (e.g. relative or staff )
- Offer earplugs or headphones, possibly with music for extra comfort
- Explain the procedure to the patient
- Instruct the patient to keep still
- Note the weight of the patient
Positioning for MRA Renal Arteries
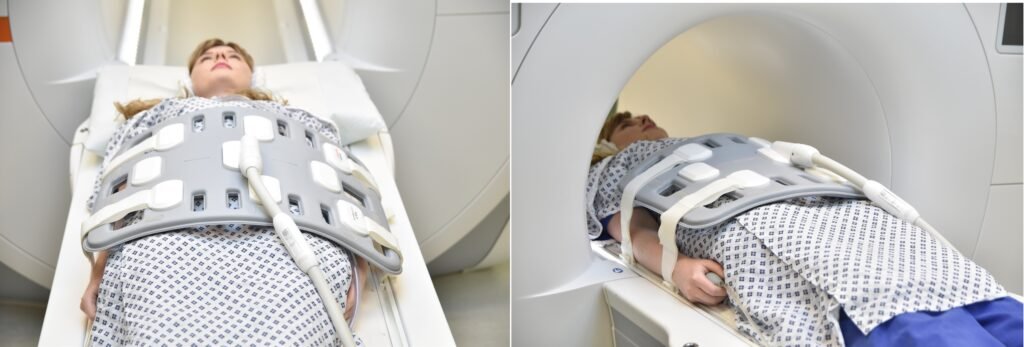
- Position the patient in supine position with head pointing towards the magnet (head first supine)
- Position the patient over the spine coil and place the body coil over the abdomen (xiphoid process down to anterior superior iliac spine)
- Securely tighten the body coil using straps to prevent respiratory artefacts
- Give a pillow under the head and cushions under the legs for extra comfort
- Centre the laser beam localiser over the level of lower intercostal border (i.e. L3 level)
Recommended MRA Renal Arteries Protocols, Parameters, and Planning
localiser
To localize and plan the sequences, it is essential to acquire a three-plane T2 HASTE localizer initially. These fast single-shot localizers have an acquisition time of under 25 seconds and are highly effective in accurately localizing abdominal structures.

T1 flash 3D coronal fat saturated .8mm -.9mm pre-contrast
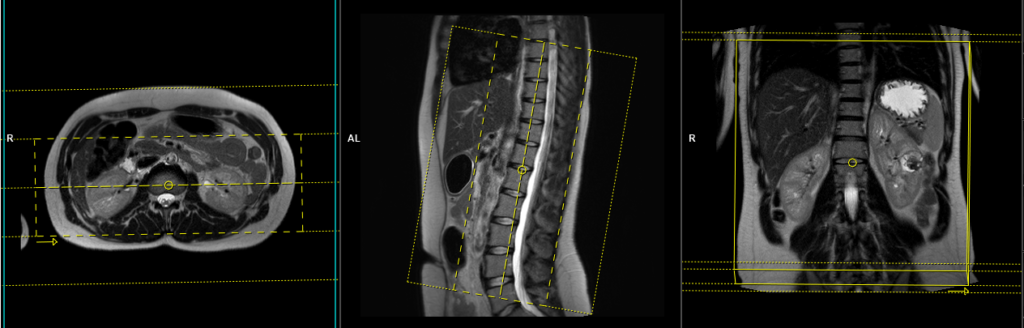
Plan the coronal slices on the axial plane; angle the positioning block horizontally across the right and left kidneys. Check the positioning block in the other two planes. An appropriate angle must be given in the sagittal plane (parallel to the abdominal aorta). Slices should be sufficient to cover both kidneys from anterior to posterior. Phase oversampling and slice oversampling should be used to avoid wrap-around artifacts. Instruct the patient to hold their breath during image acquisition. (In our department, we instruct the patients to breathe in and out twice before the “breathe in and hold” instruction.) It is highly advisable to use parallel acquisition technique to reduce the scan time (scan time should be less than 20 seconds to get the best results).

Parameters
TR 4-5 | TE 2-3 | FLIP 10 | NEX 1 | SLICE .8 MM | MATRIX 256×256 | FOV 300-350 | PHASE R>L | OVERSAMPLE 50% | IPAT ON |
Parallel acquisition technique (IPAT)
Parallel imaging is a newly developed technique used to reduce scan time without affecting the scan resolution. Using parallel acquisition MRI techniques it is possible reconstruct full-FOV images from under sampled k-space data by using the uncorrelated information from RF array coil elements. The main disadvantage of parallel acquisition techniques is the signal-to-noise ratio (SNR) is degraded because of the reduced data samples and the spatially correlated nature of multiple RF receivers.
Contrast administration and timing of scans
Guess timing technique:- This is one of the simplest methods. It works by estimating the time of contrast travel from the site of injection to the vascular structure of the abdomen. This technique is highly dependent upon the site of contrast injection, age of the patient, cardiac output, and vascular anatomy. Generally, the contrast takes about 18-25 seconds to travel from the antecubital vein to the abdominal aorta. Therefore, the post-contrast T1 acquisition should start within 20 seconds of contrast administration.
Care bolus technique:- Care bolus is the most commonly used bolus detection technique. This technique utilizes a coronal fast gradient refocused sequence to obtain real-time images of the vascular structure of interest, typically positioned over the heart, at a frequency of one image per second. The operator can observe the arrival of the contrast bolus in the heart and subsequently switch to the centric 3D sequence.
Planning care bolus
Plan the coronal care bolus slice on the sagittal plane. Position the block over the mid-heart and angle the slice parallel to the ascending aorta. Verify the position in the other two planes. Establish the appropriate angle in the axial plane, aligning it horizontally across the heart.

Care bolus scans should commence one second before contrast administration. The operator can then observe the scans in real-time and monitor the arrival of the contrast bolus in the heart. Once the contrast reaches the heart, the care bolus should be promptly halted, and the patient should be instructed to hold their breath before initiating the centric 3D dynamic sequence.

T1 flash 3D coronal fat saturated .8mm -.9mm post-contrast
Plan the coronal slices on the axial plane; angle the positioning block horizontally across the right and left kidneys. Check the positioning block in the other two planes. An appropriate angle must be given in the sagittal plane (parallel to the abdominal aorta). Slices should be sufficient to cover both kidneys from anterior to posterior. Phase oversampling and slice oversampling should be used to avoid wrap-around artifacts. Instruct the patient to hold their breath during image acquisition. (In our department, we instruct the patients to breathe in and out twice before the “breathe in and hold” instruction.) It is highly advisable to use parallel acquisition technique to reduce the scan time (scan time should be less than 20 seconds to get the best results).
Parameters
TR 4-5 | TE 2-3 | FLIP 10 | NEX 1 | SLICE .8 MM | MATRIX 256×256 | FOV 300-350 | PHASE R>L | OVERSAMPLE 50% | IPAT ON |