MRI Brachial Plexus
Indications for Brachial plexus MRI scan
- Injury to the brachial plexus is associated with weakness and paresthesias of the upper extremity on the affected side
- Pre-operative evaluation, of pathology, usually a tumour, in the region of the brachial plexus
- Pain, neural deficit or muscular atrophy possibly due to brachial plexus pathology
- Neuroma or suspected tumor
- Brachial plexopathy
- Peripheral neuropathy
- Neck injury
The brachial plexus is a network of nerves originating from the spinal cord in the neck region (C5-T1) and branching out to provide motor and sensory innervation to the upper extremities. It consists of five main branches, which are responsible for controlling movement and sensation in the shoulder, arm, forearm, and hand. Let’s explore each branch in more detail:
Musculocutaneous Nerve:
The musculocutaneous nerve innervates the muscles in the anterior compartment of the arm, including the biceps brachii, brachialis, and coracobrachialis.
It also provides sensory innervation to the lateral aspect of the forearm.
Axillary Nerve:
The axillary nerve controls the deltoid and teres minor muscles, which are involved in shoulder abduction and external rotation, respectively.
It supplies sensation to the lateral shoulder region.
Radial Nerve:
The radial nerve is the largest branch of the brachial plexus and innervates the muscles in the posterior compartment of the arm and forearm.
It controls triceps brachii, anconeus, and the extensor muscles of the forearm, enabling elbow extension and wrist extension.
Sensory branches of the radial nerve provide sensation to the posterior arm, forearm, and dorsolateral hand.
Median Nerve:
The median nerve supplies motor fibers to muscles in the anterior compartment of the forearm, including the flexor muscles of the wrist and fingers.
It also provides sensory innervation to the palmar aspect of the thumb, index, middle, and half of the ring finger.
Ulnar Nerve:
The ulnar nerve controls the muscles of the hand involved in fine motor movements, such as the flexor muscles of the ring and little fingers.
It supplies sensation to the ulnar side of the hand, including the little finger and half of the ring finger
Brachial plexus Anatomy
The brachial plexus is a network of nerves originating from the spinal cord in the neck region (C5-T1) and branching out to provide motor and sensory innervation to the upper extremities. It consists of five main branches, which are responsible for controlling movement and sensation in the shoulder, arm, forearm, and hand. Let’s explore each branch in more detail:
Musculocutaneous Nerve:
The musculocutaneous nerve innervates the muscles in the anterior compartment of the arm, including the biceps brachii, brachialis, and coracobrachialis.
It also provides sensory innervation to the lateral aspect of the forearm.
Axillary Nerve:
The axillary nerve controls the deltoid and teres minor muscles, which are involved in shoulder abduction and external rotation, respectively.
It supplies sensation to the lateral shoulder region.
Radial Nerve:
The radial nerve is the largest branch of the brachial plexus and innervates the muscles in the posterior compartment of the arm and forearm.
It controls triceps brachii, anconeus, and the extensor muscles of the forearm, enabling elbow extension and wrist extension.
Sensory branches of the radial nerve provide sensation to the posterior arm, forearm, and dorsolateral hand.
Median Nerve:
The median nerve supplies motor fibers to muscles in the anterior compartment of the forearm, including the flexor muscles of the wrist and fingers.
It also provides sensory innervation to the palmar aspect of the thumb, index, middle, and half of the ring finger.
Ulnar Nerve:
The ulnar nerve controls the muscles of the hand involved in fine motor movements, such as the flexor muscles of the ring and little fingers.
It supplies sensation to the ulnar side of the hand, including the little finger and half of the ring finger

Please check our new video tutorial for protocols and planning
Contraindications
- Any electrically, magnetically or mechanically activated implant (e.g. cardiac pacemaker, insulin pump biostimulator, neurostimulator, cochlear implant, and hearing aids)
- Intracranial aneurysm clips (unless made of titanium)
- Pregnancy (risk vs benefit ratio to be assessed)
- Ferromagnetic surgical clips or staples
- Metallic foreign body in the eye
- Metal shrapnel or bullet
Patient preparation for Brachial Plexus MRI
- A satisfactory written consent form must be taken from the patient before entering the scanner room
- Ask the patient to remove all metal objects including keys, coins, wallet, cards with magnetic strips, jewellery, hearing aid and hairpins
- If possible provide a chaperone for claustrophobic patients (e.g. relative or staff )
- Contrast injection risk and benefits must be explained to the patient before the scan
- Gadolinium should only be given to the patient if GFR is > 30
- Offer earplugs or headphones, possibly with music for extra comfort
- Explain the procedure to the patient
- Instruct the patient to keep still
- Note the weight of the patient
Positioning for Brachial Plexus MRI
- Head first supine
- Position the head in the head and neck coil and immobilise with cushions
- Give cushions under the legs for extra comfort
- Centre the laser beam localiser over the sternoclavicular joint

Recommended MRI Brachial Plexus Protocols and Planning
Brachial Plexus MRI localiser
A three-plane localizer must be taken at the beginning to localize and plan the sequences. Localizers are normally completed in less than 25 seconds and use T1-weighted low-resolution scans

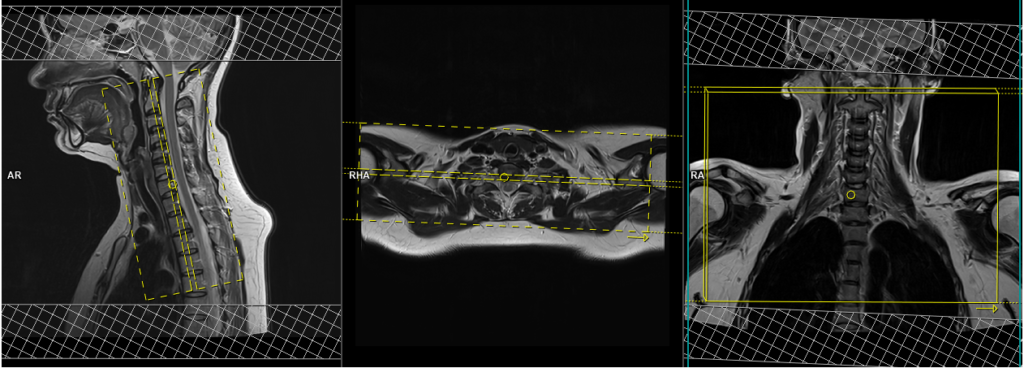
T2 stir coronal 3 mm
Plan the coronal slices on the sagittal plane and angle the positioning block parallel to the spinal cord. Verify the positioning block in the other two planes. An appropriate angle must be given in the axial plane (parallel to the right and left transverse processes of the cervical spine). The slices should adequately cover the brachial plexus from the spinous process of the cervical spine to the level of the sternoclavicular joint.
If the scanner allows a rectangular FOV, please use an FOV of 200x300mm to cover the entire brachial plexus from the right shoulder joint to the left shoulder joint. The phase direction in the coronal scans should be from right to left to avoid artifacts from chest and heart motion. It is essential to instruct the patient to avoid swallowing during sequence acquisition to prevent motion artifacts in the neck during image acquisition.
Parameters
TR 4000-6000 | TE 110 | FLIP 150 | NEX 2 | SLICE 3 MM | MATRIX 288X288 | FOV 200×300 | PHASE R>L | GAP 10% | TI 150 |
T1 tse coronal 3 mm
Plan the coronal slices on the sagittal plane and angle the positioning block parallel to the spinal cord. Verify the positioning block in the other two planes. An appropriate angle must be given in the axial plane (parallel to the right and left transverse processes of the cervical spine). The slices should adequately cover the brachial plexus from the spinous process of the cervical spine to the level of the sternoclavicular joint.
If the scanner allows a rectangular FOV, please use an FOV of 200x300mm to cover the entire brachial plexus from the right shoulder joint to the left shoulder joint. The phase direction in the coronal scans should be from right to left to avoid artifacts from chest and heart motion. It is essential to instruct the patient to avoid swallowing during sequence acquisition to prevent motion artifacts in the neck during image acquisition.

Parameters
TR 500-600 | TE 15-25 | SLICE 3 MM | FLIP 150 | PHASE R>L | MATRIX 330X320 | FOV 200×300 | GAP 10% | NEX(AVRAGE) 2 |
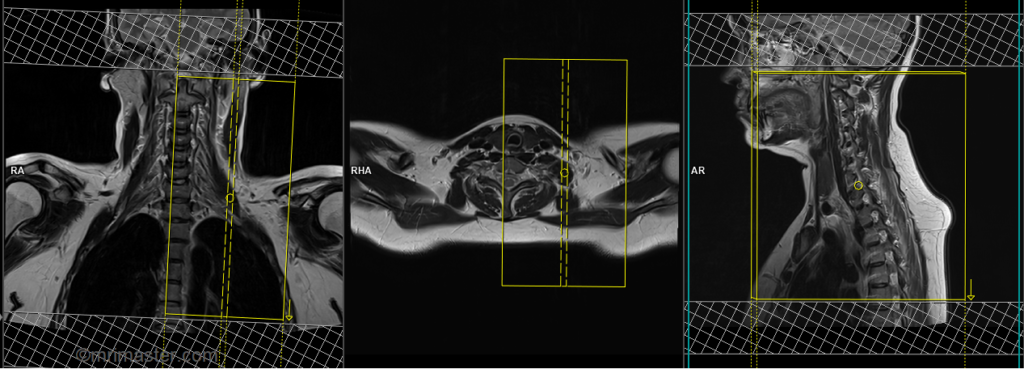
T1 tse axial 3mm
Plan the axial slices on the sagittal plane and angle the positioning block perpendicular to the spinal cord. Check the positioning block in the other two planes, ensuring an appropriate angle is given in the coronal plane (perpendicular to the cervical spine). The slices must be sufficient to cover the brachial plexus from C3 down to the level of T4, and the field of view (FOV) must be big enough to encompass the entire brachial plexus from the right shoulder joint to the left shoulder joint.
For the axial scans, the phase direction must be right to left with 100% oversample. This will help reduce arterial pulsation and swallowing artifacts. It is important to instruct the patient to avoid swallowing during sequence acquisition to prevent motion artifacts in the neck during image acquisition.

Parameters
TR 400-600 | TE 15-25 | SLICE 3 MM | FLIP 150 | PHASE A>P | MATRIX 384X384 | FOV 320-350 | GAP 10% | NEX(AVRAGE) 2 |
T2 STIR axial 3mm
Plan the axial slices on the sagittal plane and angle the positioning block perpendicular to the spinal cord. Check the positioning block in the other two planes, ensuring an appropriate angle is given in the coronal plane (perpendicular to the cervical spine). The slices must be sufficient to cover the brachial plexus from C3 down to the level of T4, and the field of view (FOV) must be big enough to encompass the entire brachial plexus from the right shoulder joint to the left shoulder joint.
For the axial scans, the phase direction must be right to left with 100% oversample. This will help reduce arterial pulsation and swallowing artifacts. It is important to instruct the patient to avoid swallowing during sequence acquisition to prevent motion artifacts in the neck during image acquisition.
Parameters
TR 4000-5000 | TE 110 | FLIP 150 | NEX 2 | SLICE 3 MM | MATRIX 384X320 | FOV 320-350 | PHASE A>P | GAP 10% | TI 150 |
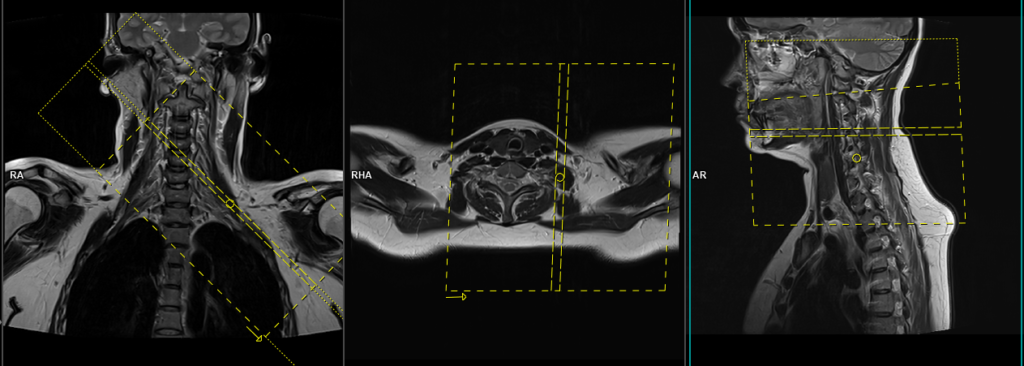
T2 tse sagittal 3 mm SFOV affected side
Plan the sagittal slices on the coronal plane, angling the positioning block parallel to the cervical spine. Check the positioning block in the other two planes, ensuring an appropriate angle is given in the axial plane (parallel to the vertebral body and transverse process). The slices must be sufficient to cover the affected side (right or left) from the spinal cord out to the shoulder joint. The phase direction in the sagittal scans can be head to feet with 100-150% oversample to reduce arterial pulsation and swallowing artifacts. It is essential to instruct the patient to avoid swallowing during sequence acquisition to prevent motion artifacts during image acquisition.
Parameters
TR 4000-5000 | TE 110 | FLIP 150 | NEX 2 | SLICE 3 MM | MATRIX 320X320 | FOV 200-230 | PHASE H>F | GAP 10% | oversample 100% |
T2 stir sagittal oblique 3 mm SFOV affected side
Plan the sagittal oblique slices on the coronal plane, angling the positioning block perpendicular to the brachial plexus. Check the positioning block in the other two planes. An appropriate angle must be given in the axial plane (parallel to the vertebral body and transverse process). Slices must be sufficient to cover the affected side (right or left) from the spinal cord out to the shoulder joint. The phase direction in the sagittal scans can be head to feet with 100-150% oversample. This will reduce arterial pulsation and swallowing artifacts. It is important to instruct the patient to avoid swallowing during sequence acquisition to avoid motion artifacts in the neck during image acquisition.

Parameters
TR 4000-5000 | TE 110 | FLIP 130 | NEX 2 | SLICE 3 MM | MATRIX 320X256 | FOV 200-230 | PHASE H>F | GAP 10% | TI 130 |
T2 TSE AXIAL oblique 3 mm SFOV affected side
Plan the axial oblique slices on the coronal plane and angle the positioning block parallel to the brachial plexus. Check the positioning block in the other two planes. An appropriate angle must be given in the sagittal plane (perpendicular to the spinal cord). The slices must be sufficient to cover the affected side (right or left) from C3 to T3. The phase direction in the sagittal scans can be right to left with 100-150% oversample. This will reduce arterial pulsation and swallowing artifacts. It is important to instruct the patient to avoid swallowing during sequence acquisition to avoid motion artifacts in the neck during image acquisition.
Parameters
TR 4000-5000 | TE 110 | FLIP 150 | NEX 2 | SLICE 3 MM | MATRIX 320X320 | FOV 200-230 | PHASE R>L | GAP 10% | oversample 100% |
Rarely do brachial plexus scans require contrast-enhanced imaging. In this case, use T1 TSE DIXON axial and coronal sequences after the administration of IV gadolinium DTPA injection (copy the planning outlined above). The document below provides access to the recommended dosage of gadolinium DTPA injection, as advised by the manufacturer.