Large Pelvic and Abdominal Mass MRI Protocol and Planning
Indications for MRI Large Pelvic and Abdominal Mass scans
- Large ovarian cyst
- Large ovarian tumors
- Large fibroids
- large abdominal tumors
- Abdominal infections
Contraindications
- Any electrically, magnetically or mechanically activated implant (e.g. cardiac pacemaker, insulin pump biostimulator, neurostimulator, cochlear implant, and hearing aids)
- Intracranial aneurysm clips (unless made of titanium)
- Pregnancy (risk vs benefit ratio to be assessed)
- Ferromagnetic surgical clips or staples
- Metallic foreign body in the eye
- Metal shrapnel or bullet
Patient preparation for MRI Large Pelvic and Abdominal Mass scans
- A satisfactory written consent form must be taken from the patient before entering the scanner room
- Ask the patient to remove all metal objects including keys, coins, wallet, cards with magnetic strips, jewellery, hearing aid and hairpins
- Ask the patient to undress and change into a hospital gown
- Contrast and buscopan injection risk and benefits must be explained to the patient before the scan
- Gadolinium should only be given to the patient if GFR is > 30
- An intravenous line must be placed with extension tubing extending out of the magnetic bore
- Claustrophobic patients may be accompanied into the scanner room e.g. by staff member or relative with proper safety screening
- Offer earplug or headphones possibly with music for extra comfort.
- Explain the procedure to the patient and answer questions
- Note down the weight of the patient
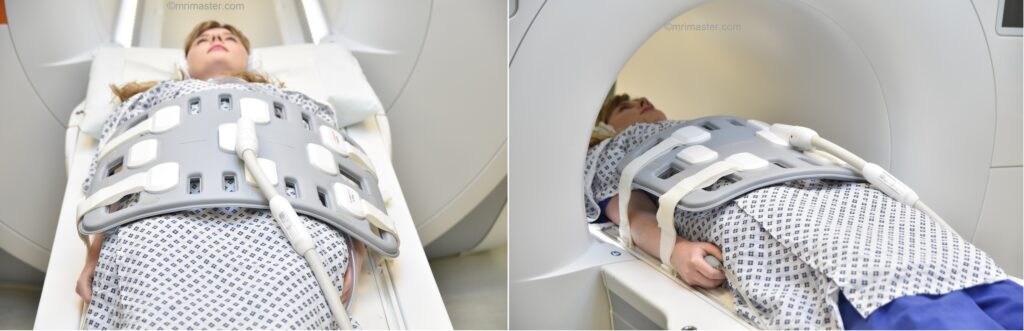
Positioning for MRI Large Pelvic and Abdominal Mass scans
- Position the patient in supine position with head pointing towards the magnet (head first supine)
- Position the patient over the spine coil and place the body coil over abdomen and pelvis (nipple down to three inches below symphysis pubis)
- Securely tighten the body coil using straps to prevent respiratory artefacts
- Give a pillow under the head and cushions under the legs for extra comfort
- Centre the laser beam localiser over the iliac crest
- Register the patient in the scanner as head first supine
Recommended MRI Large Pelvic and Abdominal Mass scan Protocols and Planning
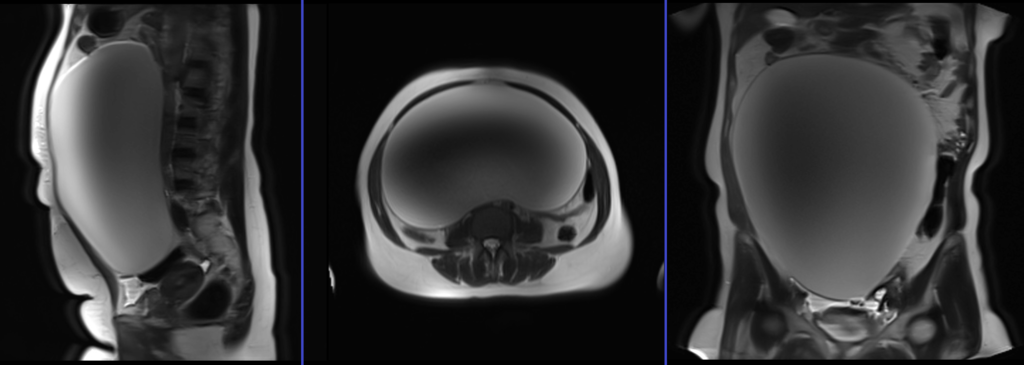
MRI localiser
A three-plane localiser must be taken at the beginning to localise and plan the sequences. Localisers are normally less than 25 seconds and are T2-weighted low-resolution scans.
Pause for buscopan injection
Before proceeding to the next step, intravenously inject 0.5 to 1 ml of Buscopan (according to the manufacturer’s instructions and departmental policy). Wait for 1 minute before starting the next scan (Buscopan takes a few seconds to start its function).
Warning
* Buscopan injection should not be administered to patients with myasthenia gravis, megacolon, narrow angle glaucoma, tachycardia, prostatic enlargement with urinary retention, mechanical stenoses in the region of the gastrointestinal tract or paralytic ileus.*
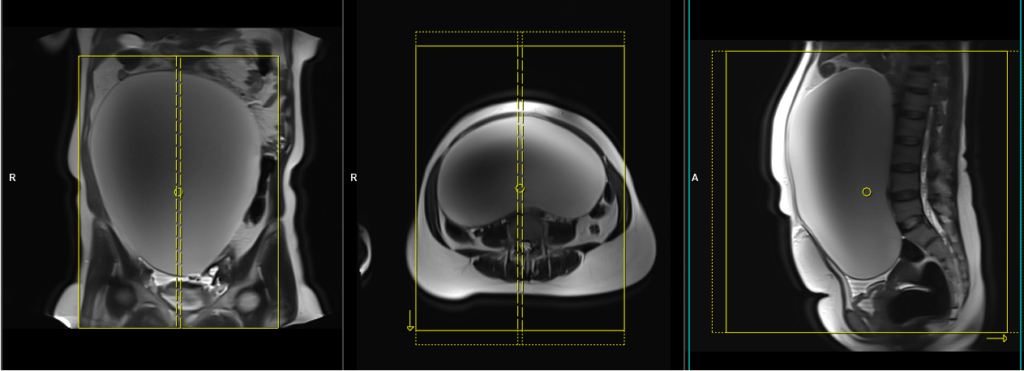
T2 tse sagittal large FOV 4mm multiple breath hold / respiratory gated
Plan the sagittal slices on the coronal plane and align the positioning block vertically across the abdomen. Verify the positioning block in the other two planes. In the axial plane, plan the block vertically across the abdomen as shown. Ensure that the slices cover the entire pelvic and abdominal mass, extending from the right to the left. The field of view (FOV) should be sufficiently large to encompass the mass, typically ranging from 350mm to 400mm. Ensure an adequate level of phase oversampling to prevent any wrap-around artifacts.
Due to the large number of slices, the scan is split into three breath-hold acquisitions, each around 20 seconds long. Instruct the patient to hold their breath during the image acquisition. If T2 TSE scans are not available on your scanner, please use TSE-based single-shot sequences (e.g., HASTE). If the patient is unable to hold their breath, consider using respiratory-gated sequences or radial k-space sequences (e.g., BLADE T2)
Parameters
TR 4000-5000 | TE 100-120 | SLICE 4 MM | FLIP 130-150 | PHASE A>P | MATRIX 320X320 | FOV 350-400 | GAP 10% | NEX(AVRAGE) 2 |
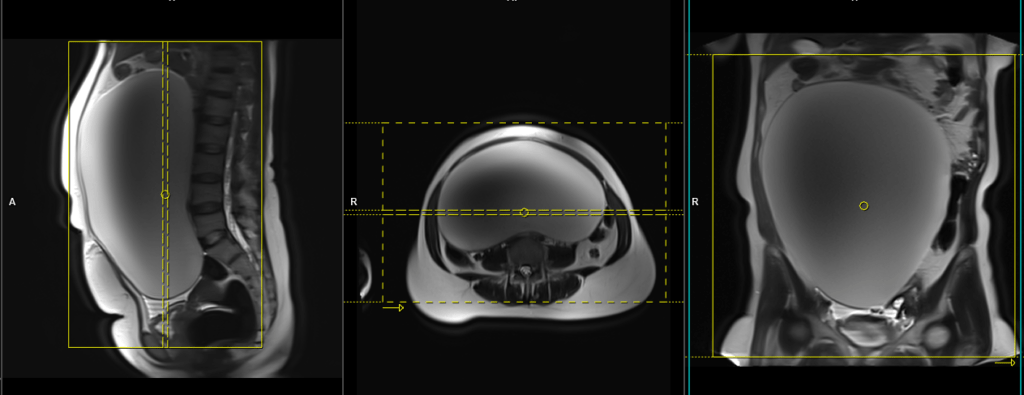
T2 tse axial large FOV 5mm multiple breath hold / respiratory gated
Plan the large field of view (FOV) T2 axial slices on the coronal plane, positioning the block parallel to the line along the right and left iliac crest. Verify the positioning block in the other two planes as well. Establish an appropriate angle in the sagittal plane, perpendicular to the lumbar spine. Ensure that the slices cover the entire pelvic and abdominal mass from top to bottom. The field of view (FOV) should be sufficiently large to encompass the mass, typically ranging from 350mm to 400mm. Use right-to-left phase direction with an adequate level of phase oversampling to prevent any wrap-around artifacts.
Due to the large number of slices, the scan is split into four breath-hold acquisitions, each around 20 seconds long. Instruct the patient to hold their breath during the image acquisition. If T2 TSE scans are not available on your scanner, please use TSE-based single-shot sequences (e.g., HASTE). If the patient is unable to hold their breath, consider using respiratory-gated sequences or radial k-space sequences (e.g., BLADE T2). Using saturation bands above and below the planning block can minimize breathing, pulsation, and peristalsis-related artifacts.

Parameters
TR 4000-5000 | TE 100-120 | SLICE 5 MM | FLIP 130-150 | PHASE R>L | MATRIX 320X320 | FOV 350-400 | GAP 10% | NEX(AVRAGE) 2 |
T1 tse axial large FOV 5mm multiple breath hold / respiratory gated
Plan the large field of view (FOV) T1 axial slices on the coronal plane, positioning the block parallel to the line along the right and left iliac crest. Verify the positioning block in the other two planes as well. Establish an appropriate angle in the sagittal plane, perpendicular to the lumbar spine. Ensure that the slices cover the entire pelvic and abdominal mass from top to bottom. The field of view (FOV) should be sufficiently large to encompass the mass, typically ranging from 350mm to 400mm. Use right-to-left phase direction with an adequate level of phase oversampling to prevent any wrap-around artifacts.
Due to the large number of slices, the scan is split into four breath-hold acquisitions, each around 20 seconds long. Instruct the patient to hold their breath during the image acquisition. If the patient is unable to hold their breath, consider using respiratory-gated sequences or radial k-space sequences (e.g., BLADE T1). Using saturation bands above and below the planning block can minimize breathing, pulsation, and peristalsis-related artifacts.
Parameters
TR 400-600 | TE 15-25 | SLICE 5 MM | FLIP 130 | PHASE R>L | MATRIX 320X320 | FOV 350-400 | GAP 10% | NEX(AVRAGE) 2 |
T1 tse fat saturated large FOV 5mm free breathing
Plan the large field of view (FOV) T1 fat saturated axial slices on the coronal plane, positioning the block parallel to the line along the right and left iliac crest. Verify the positioning block in the other two planes as well. Establish an appropriate angle in the sagittal plane, perpendicular to the lumbar spine. Ensure that the slices cover the entire pelvic and abdominal mass from top to bottom. The field of view (FOV) should be sufficiently large to encompass the mass, typically ranging from 350mm to 400mm. Use right-to-left phase direction with an adequate level of phase oversampling to prevent any wrap-around artifacts. Instruct the patient to breathe gently during the image acquisition. Using saturation bands above and below the planning block can minimize breathing, pulsation, and peristalsis-related artifacts.
Parameters
TR 400-600 | TE 15-25 | SLICE 5 MM | FLIP 130 | PHASE R>L | MATRIX 320X320 | FOV 350-400 | GAP 10% | NEX(AVRAGE) 2 |
EPI DWI (b0-b500-b1000)large FOV 5mm free breathing
Plan the large field of view (FOV) EPI DWI axial slices on the coronal plane, positioning the block parallel to the line along the right and left iliac crest. Verify the positioning block in the other two planes as well. Establish an appropriate angle in the sagittal plane, perpendicular to the lumbar spine. Ensure that the slices cover the entire pelvic and abdominal mass from top to bottom. The field of view (FOV) should be sufficiently large to encompass the mass, typically ranging from 350mm to 400mm. Use right-to-left phase direction with an adequate level of phase oversampling to prevent any wrap-around artifacts. Instruct the patient to breathe gently during the image acquisition. Using saturation bands above and below the planning block can minimize breathing, pulsation, and peristalsis-related artifacts.
Parameters
TR 6000-7000 | TE 90 | IPAT ON | NEX 3 5 8 | SLICE 5 MM | MATRIX 208X208 | FOV 350-400 | PHASE R>L | GAP 10% | B VALUE 0 |
T2 tse coronal large FOV 4mm multiple breath hold / respiratory gated
Plan the coronal T2 TSE slices on the sagittal plane and align the positioning block vertically across the abdomen. Verify the positioning block in the other two planes. In the axial plane, plan the block horizontally across the abdomen, as shown. Ensure that the slices cover the entire pelvic and abdominal mass, extending from the anterior to the posterior. The field of view (FOV) should be sufficiently large to encompass the mass, typically ranging from 350mm to 400mm. Use a right-to-left phase direction with an adequate level of phase oversampling to prevent any wrap-around artifacts.
Due to the large number of slices, the scan is split into three breath-hold acquisitions, each approximately 20 seconds long. Instruct the patient to hold their breath during image acquisition. If T2 TSE scans are unavailable on your scanner, please use TSE-based single-shot sequences (e.g., HASTE). If the patient is unable to hold their breath, consider using respiratory-gated sequences or radial k-space sequences (e.g., BLADE T2).
Parameters
TR 4000-5000 | TE 100-120 | SLICE 4 MM | FLIP 130-150 | PHASE R>L | MATRIX 320X320 | FOV 350-400 | GAP 10% | NEX(AVRAGE) 2 |
STIR large FOV 5mm BLADE free breathing / respiratory gated
Plan the coronal T2 TSE slices on the sagittal plane and align the positioning block vertically across the abdomen. Verify the positioning block in the other two planes. In the axial plane, plan the block horizontally across the abdomen, as shown. Ensure that the slices cover the entire pelvic and abdominal mass, extending from the anterior to the posterior. The field of view (FOV) should be sufficiently large to encompass the mass, typically ranging from 350mm to 400mm. Use a right-to-left phase direction with an adequate level of phase oversampling to prevent any wrap-around artifacts. Instruct the patient to breathe gently during the image acquisition. Use free breathing respiratory-gated sequences or radial k-space sequences (e.g., BLADE T2).
Parameters
TR 4000-5000 | TE 110 | FLIP 130 | NEX 2 | SLICE 5MM | MATRIX 384X320 | FOV 380-400 | PHASE R>L | GAP 10% | TI 130 |
T1 VIBE DIXON 3D 4mm coronal dynamic 1 pre 8 post free breathing
Plan the coronal T1 VIBE DIXON 3D block on the sagittal plane and align the positioning block vertically across the abdomen. Verify the positioning block in the other two planes. In the axial plane, plan the block horizontally across the abdomen, as shown. Ensure that the slices cover the entire pelvic and abdominal mass, extending from the anterior to the posterior. The field of view (FOV) should be sufficiently large to encompass the mass, typically ranging from 350mm to 400mm. Use a right-to-left phase direction with an adequate level of phase oversampling to prevent any wrap-around artifacts. Instruct the patient to breathe gently during the image acquisition. Use free breathing respiratory-gated sequences or radial k-space sequences (e.g., BLADE T2).

Parameters
TR 4-5 | TE 2-3 | FLIP 10 | NEX 1 | SLICE 4 MM | MATRIX 384X320 | FOV 350-400 | PHASE R>L | DYNAMIC 9 SCANS | IPAT ON |