MRI Shoulder ABER (Abduction and External Rotation) view
What is ABER View?
The ABER (Abduction and External Rotation) view in MRI is a specialized imaging sequence used primarily in shoulder MR arthrography to evaluate the glenohumeral joint and surrounding structures under stress. In this position, the patient’s arm is abducted (moved away from the body) and externally rotated, mimicking the “cocking” phase of a throwing motion, which places stress on certain structures in the shoulder.
The ABER view is particularly useful for visualizing:
- Glenoid labrum (especially the anteroinferior labrum).
- Supraspinatus tendon (undersurface and articular side).
- Inferior glenohumeral ligament (anterior band).
By positioning the shoulder in this manner, the ABER sequence helps reveal conditions that might not be visible in a neutral position, such as labral tears, rotator cuff tears, or capsular injuries. The view stresses the anterior and inferior structures of the shoulder joint, making it highly valuable in assessing conditions like SLAP tears, Bankart lesions, or rotator cuff pathologies.
Indications for shoulder MRI scan
- Assessment of the Inferior Glenohumeral Ligament
- Evaluation of Shoulder Impingement
- Evaluation of Labral Tears
- Postoperative Assessment
- Glenohumeral Instability
- Rotator Cuff Pathologies
Contraindications
- Any electrically, magnetically or mechanically activated implant (e.g. cardiac pacemaker, insulin pump biostimulator, neurostimulator, cochlear implant, and hearing aids)
- Intracranial aneurysm clips (unless made of titanium)
- Pregnancy (risk vs benefit ratio to be assessed)
- Ferromagnetic surgical clips or staples
- Metallic foreign body in the eye
- Metal shrapnel or bullet
Patient preparation for shoulder MRI
- A satisfactory written consent form must be taken from the patient before entering the scanner room
- Ask the patient to remove all metal objects including keys, coins, wallet, cards with magnetic strips, jewellery, hearing aid and hairpins
- If possible provide a chaperone for claustrophobic patients (e.g. relative or staff )
- Offer earplugs or headphones, possibly with music for extra comfort
- Explain the procedure to the patient
- Instruct the patient to keep still
- Note the weight of the patient
Positioning for shoulder MRI
- Patient lies supine on the MRI scanner table with their affected arm abducted and externally rotated. Ideally, the arm should be in 90° abduction and 90° external rotation, although this position may need to be adjusted depending on patient comfort and the MRI machine’s closed-bore configuration. Often, more than 90° of abduction is required to accommodate the arm within the MRI bore.
- Now, wrap the flex coil around the shoulder as shown in the photos.
- Centre the laser beam localiser over the shoulder joint or the mid line of the coil
- Register the patient on the scanner as 'head first supine'

Recommended MRI ABER view positioning Protocols, Parameters, and Planning
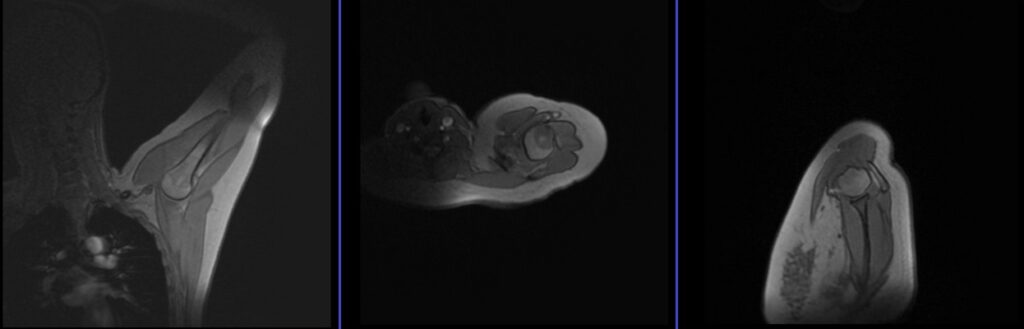
localiser
A three-plane localizer must be taken at the beginning to localize and plan the sequences. Typically, localizers take less than 25 seconds and utilize T1 weighted low-resolution scans for this purpose.
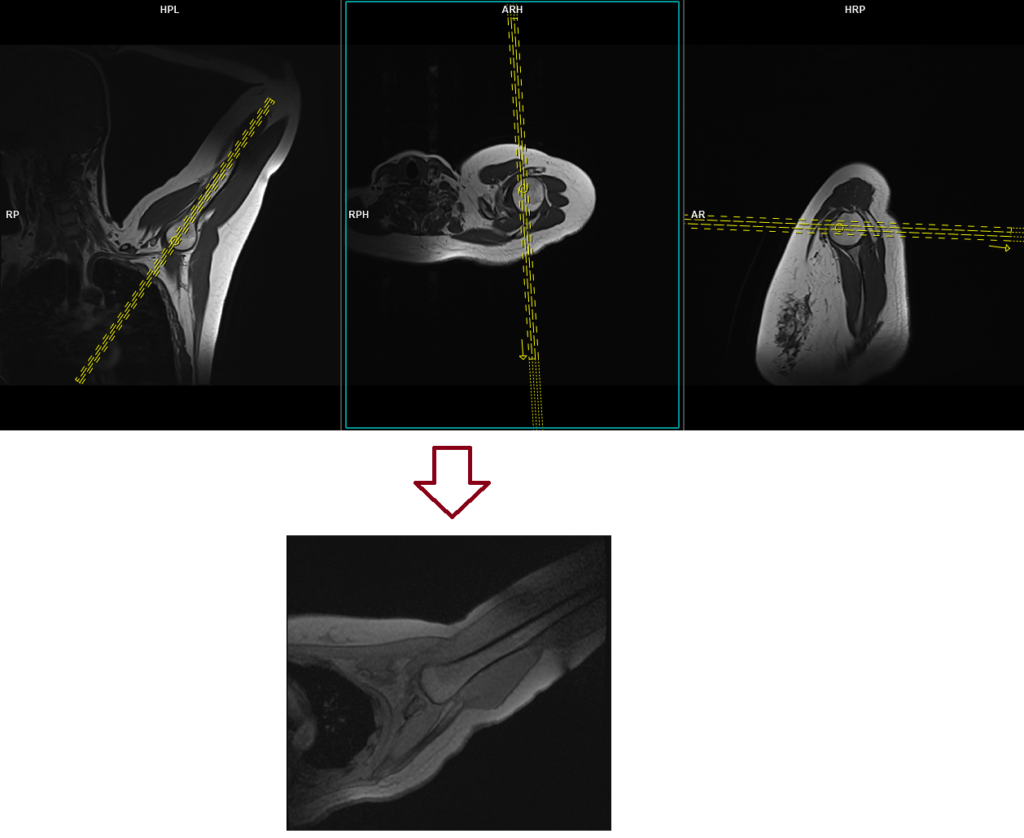
localiser axial oblique
Plan the axial oblique localizer scan on the coronal plane and align the positioning block parallel to the humerus. Verify the positioning block in the other two planes. In the sagittal plane, use an angle perpendicular to the humeral head or scapula blade, and in the axial plane, ensure it is parallel to the glenoid labrum.
localiser sagittal oblique
Plan the sagittal oblique localizer scan on the coronal plane and align the positioning block perpendicular to the humeral head. Check the positioning block in the other two planes as well. In the axial oblique plane, adjust the angle to be perpendicular to the humeral head or scapula blade, and in the axial plane, make sure it is parallel to the glenoid labrum.

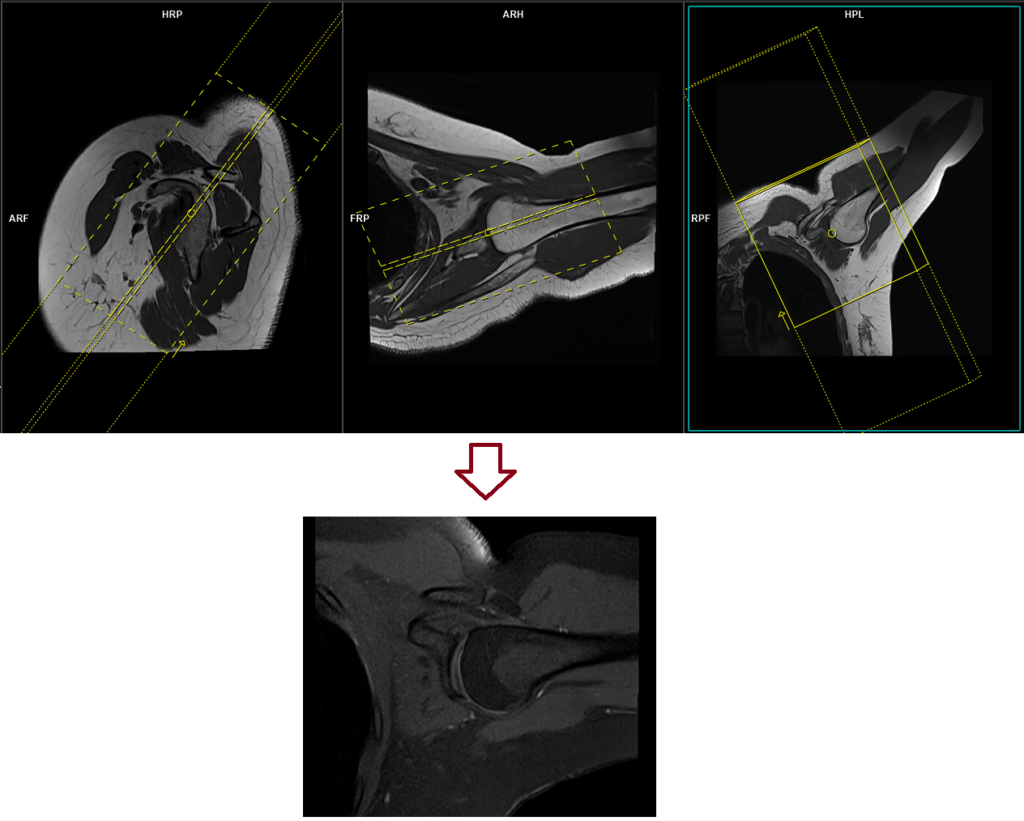
T1 tse SPAIR coronal oblique 3mm SFOV
Plan the coronal oblique slices on the sagittal plane, and align the positioning block parallel to the supraspinatus tendon and the anterior-inferior aspect of the glenoid labrum. Check the positioning block’s alignment in the other two planes. Set the angle in the axial oblique plane to be parallel with the humeral head. Ensure that the slices encompass the entire shoulder joint, from the anterior to the posterior.
Parameters
TR 600-700 | TE 15-25 | SLICE 3 MM | FAT SAT SPAIR | PHASE A>P | MATRIX 256X256 | FOV 130-160 | GAP 10% | NEX(AVRAGE) 2 |