MRA Hand(Dynamic) : Protocol and Planning
Indications for MRA hand
- Thrombotic and embolic disease
- Arteriovenous malformation
- Atherosclerotic disease
- Artery dissections
- Vein thrombosis
- Artery stenosis
- Aneurysms
- Vasculitis
- Vasospasm
Contraindications
- Any electrically, magnetically or mechanically activated implant (e.g. cardiac pacemaker, insulin pump biostimulator, neurostimulator, cochlear implant, and hearing aids)
- Intracranial aneurysm clips (unless made of titanium)
- Pregnancy (risk vs benefit ratio to be assessed)
- Ferromagnetic surgical clips or staples
- Metallic foreign body in the eye
- Metal shrapnel or bullet
Patient preparation
- A satisfactory written consent form must be taken from the patient before entering the scanner room
- Ask the patient to remove all metal objects including keys, coins, wallet, cards with magnetic strips, jewellery, hearing aid and hairpins
- Contrast injection risk and benefit must be explained to the patient before the scan.
- Gadolinium should only be given to the patient if GFR is > 30
- Intravenous line must be placed in the unaffected side e.g if the problem exists in RT arm the canula should be in LT side
- An intravenous line must be placed with extension tubing extending out of the magnetic bore
- Claustrophobic patients may be accompanied into the scanner room e.g. by staff member or relative with proper safety screening
- Offer headphones for communicating with the patient and ear protection
- Explain the procedure to the patient and answer questions
- Note the weight of the patient
Positioning for MRA Hand
- Head first prone with arm up (superman position)
- Position the hand in large flex coil and immobilize with cushions
- Give cushions under the chest for extra comfort
- Centre the laser beam localiser over the metacarpophalangeal joint
- Register the patient in the scanner as head first supine

Recommended MRA Hand Protocols and Planning
Localiser
A three-plane localizer must be taken at the beginning to localize and plan the sequences. Typically, these localizers take less than 25 seconds and can be achieved using T1 weighted low-resolution scans. It is advisable to obtain additional localizers until you have acquired accurate axial, coronal, and sagittal localizer images.
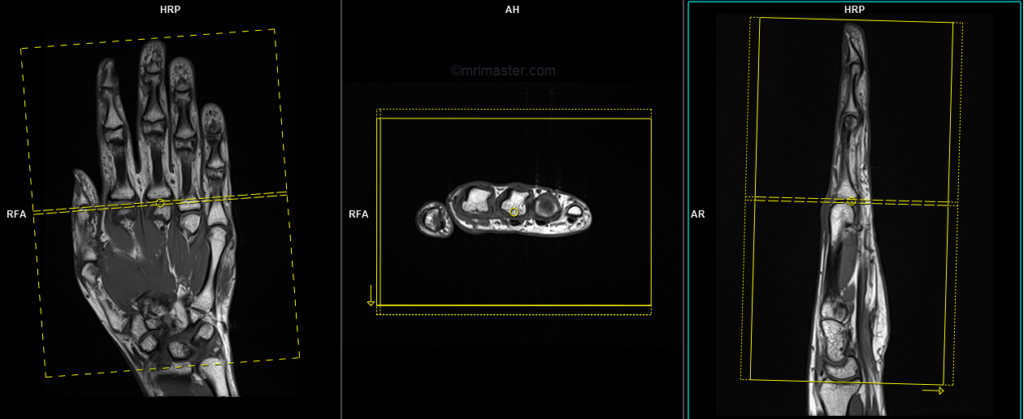
T1 vibe 3D fat sat axial 2mm small fov pre-contrast
Plan the axial slices on the coronal localizer and angle the positioning block perpendicular to the metacarpal and phalangeal bones. Check the positioning block in the other two planes. Ensure an appropriate angle is used in the sagittal plane, perpendicular to the metacarpal and phalangeal bones. The slices should adequately cover the entire hand, spanning from the fingertip to the line of the distal radioulnar joint.
Parameters
TR 4-5 | TE 2 | FLIP 12 | NEX 3 | SLICE 2 MM | MATRIX 256X256 | FOV 160 | PHASE A>P | OVERSAMPLE nil | IPAT Off |
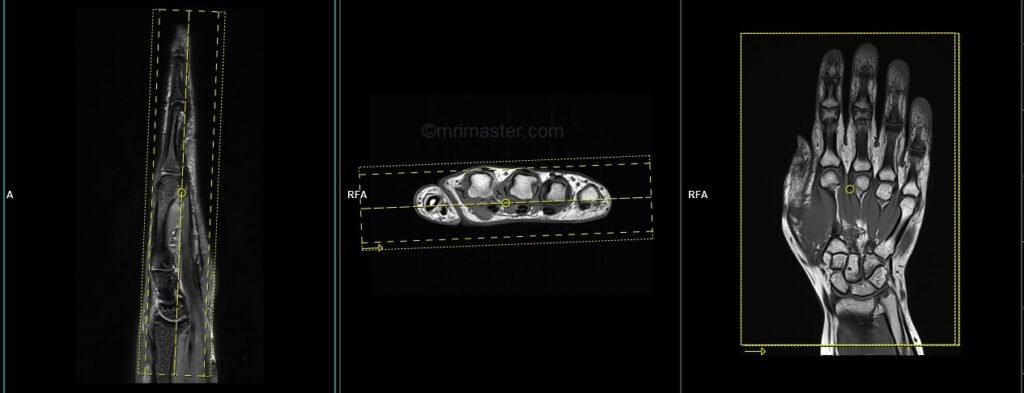
T1 flash 3D fat sat coronal .8mm -1 mm pre-contrast
Plan the coronal slices on the axial plane and position the block horizontally across the metacarpal bones. Check the positioning block in the other two planes. An appropriate angle must be used in the sagittal plane, parallel to the metacarpal and phalangeal bones. The slices should sufficiently cover the entire hand, from the dorsal aspect to the palmar aspect. The scan acquisition time should be less than 10 seconds to achieve the best results.
Parameters
TR 4-5 | TE 2-3 | FLIP 10 | NEX 1 | SLICE .8 MM | MATRIX 256×256 | FOV 200-250 | PHASE R>L | OVERSAMPLE 50% | IPAT Off |
contrast administration and timing of scans
Guess timing technique:-
This is one of the simplest techniques used in MRA. It involves estimating the time it takes for contrast to travel from the injection site to the vascular structure of the abdomen. The effectiveness of this technique relies heavily on factors such as the site of contrast injection, the patient’s age, cardiac output, and vascular anatomy.
Typically, it takes approximately 15-20 seconds for the contrast to travel from the antecubital vein to the arch of the aorta, and an additional 20-30 seconds to reach the hand. Therefore, the post-contrast T1 acquisition should commence after 35 seconds of contrast administration.
The guess timing technique is particularly useful for MRA of the hands, as each acquisition takes less than 8 seconds, enabling us to obtain both the arterial and venous phases effectively.
T1 flash dynamic 3D fat sat coronal .8mm - 1mm post-contrast 15 measurement
Plan the coronal slices on the axial plane and position the block horizontally across the metacarpal bones. Check the positioning block in the other two planes. An appropriate angle must be used in the sagittal plane, parallel to the metacarpal and phalangeal bones. The slices should sufficiently cover the entire hand, from the dorsal aspect to the palmar aspect. The scan acquisition time should be less than 10 seconds to achieve the best results.
Parameters
TR 4-5 | TE 2-3 | FLIP 10 | NEX 1 | SLICE .8 MM | MATRIX 256×256 | FOV 200-250 | PHASE R>L | OVERSAMPLE 50% | dynamic 15 |
In order for subtraction of the images to be possible, it is crucial that the measurements of pre and post contrast T1 scans are identical. Any differences in slice thickness, FOV, or planning would hinder the ability to perform image subtraction.
T1 vibe 3D fat sat axial 2mm small fov post-contrast
Plan the axial slices on the coronal localizer and angle the positioning block perpendicular to the metacarpal and phalangeal bones. Check the positioning block in the other two planes. Ensure an appropriate angle is used in the sagittal plane, perpendicular to the metacarpal and phalangeal bones. The slices should adequately cover the entire hand, spanning from the fingertip to the line of the distal radioulnar joint.
Parameters
TR 4-5 | TE 2 | FLIP 12 | NEX 3 | SLICE 2 MM | MATRIX 256X256 | FOV 160 | PHASE A>P | OVERSAMPLE nil | IPAT Off |