MRI Spinal Cord : Protocol and Planning
Indications for MRI Spinal Cord
- Evaluation or monitoring of congenital malformations of the spinal cord
- Evaluation or monitoring of inflammation of the CNS or meninges
- Multiple Sclerosis or other demyelinating diseases
- Spinal Cord Tumour
- Syringomyelia
- Spinal cord AVM
Contraindications
- Any electrically, magnetically or mechanically activated implant (e.g. cardiac pacemaker, insulin pump biostimulator, neurostimulator, cochlear implant, and hearing aids)
- Intracranial aneurysm clips (unless made of titanium)
- Pregnancy (risk vs benefit ratio to be assessed)
- Ferromagnetic surgical clips or staples
- Metallic foreign body in the eye
- Metal shrapnel or bullet
Patient preparation for MRI Spinal Cord
- A satisfactory written consent form must be taken from the patient before entering the scanner room
- Ask the patient to remove all metal objects including keys, coins, wallet, cards with magnetic strips, jewellery, hearing aid and hairpins
- If possible provide a chaperone for claustrophobic patients (e.g. relative or staff )
- Contrast injection risk and benefits must be explained to the patient before the scan
- Gadolinium should only be given to the patient if GFR is > 30
- Offer earplugs or headphones, possibly with music for extra comfort
- Explain the procedure to the patient
- Instruct the patient to keep still
- Note the weight of the patient
Positioning for MRI Spinal Cord
- Position patient in the supine position with the head pointing towards the magnet (head first supine)
- Position the patient in the spine, head, and neck coil, and place the head and neck coil over the head.
- Give cushions under the legs for extra comfort
- Centre the laser beam localiser over the sternoclavicular joint for upper cord planning

Recommended MRI Spinal Cord Protocols and Planning
localiser cervicothoracic spine
A three plane localiser must be taken in the beginning to localise and plan the sequences. Localisers are normally less than 25 seconds long and are T1 weighted low resolution scans.

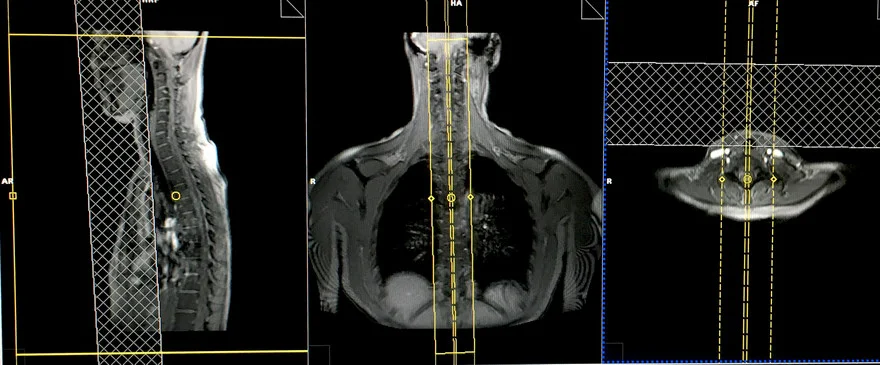
T2 tse sagittal large FOV localiser for spine counting
This scan is for the localisation of the spinal cord and to check the vertebral body level of any spinal cord pathologies. This sequence can be performed under one minute with a limited number of slices and parallel imaging techniques. The alternative to this method is to perform the scans with a marker such as a cod liver oil tablet placed at the level of T4. The marker must be included in the upper and lower spinal cord high resolution small field of view (FOV) sagittal scans.
Plan the sagittal slices on the coronal plane, angle the position block parallel to the spinal cord. Check the positioning block in the other two planes. An appropriate angle must be given in the axial plane on a tilted patient, this should be parallel to the imaginary line running through the centre of the vertebral body and spinous process. Check the position block in the sagittal plane where the FOV must be big enough to cover the whole cervical and thoracic spine from C1 down to T12. An FOV of 480mm should normally be sufficient. The slices should be enough to cover the spine from the lateral border of the right transverse process to the lateral border of left transverse process. A saturation band must be placed over the chest in the sagittal plane to avoid breathing artefacts over the spinal area. The phase direction should be head to foot to avoid further motion artefacts from the chest.
Parameters
TR 3000-4000 | TE 100-120 | SLICE 4MM | IPAT ON | PHASE H>F | MATRIX 512X384 | FOV 480-490 | GAP 10% | NEX(AVRAGE) 1 |
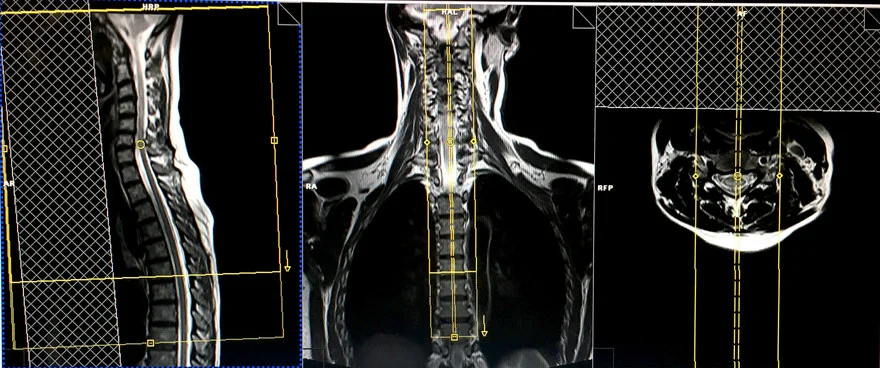
T2 tse sagittal 2mm 270-280 FOV or Isotropic 3D T2 SPACE .9mm
Utilising thin slices and small field of views is mandatory for spinal cord imaging to enable the detection of small multiple sclerosis (MS) lesions. The modern practise is to replace the tse scans with an isotropic 3D sequence with a slice thickness of 0.9mm.
Plan the sagittal slices on the coronal plane, angle the position block parallel to spinal cord. Check the positioning block in the other two planes. An appropriate angle must be given in the axial plane on a tilted patient, this should be parallel to the imaginary line running through the centre of the vertebral body and the spinous process. Check the position block in the sagittal plane where the FOV must be big enough to cover the upper spinal cord from the pons down to T5. Normally an FOV of 270- 280mm should be sufficient. The slices should be enough to cover the spinal cord side to side. A saturation band must be placed over the neck in front of the oesophagus in the sagittal plane to avoid swallowing artefacts. The phase direction should be head to foot to avoid motion artefacts from the neck.
Parameters
TR 3000-4000 | TE 110 | SLICE 2MM | FLIP 130-150 | PHASE H>F | MATRIX 320X320 | FOV 270-280 | GAP 10% | NEX(AVRAGE) 4 |
T1 tse sagittal 2mm 270-280 FOV or Isotropic 3D T1 .9mm
Plan the sagittal slices on the coronal plane, angle the position block parallel to spinal cord. Check the positioning block in the other two planes. An appropriate angle must be given in the axial plane on a tilted patient, this should be parallel to the imaginary line running through the centre of the vertebral body and the spinous process. Check the position block in the sagittal plane where the FOV must be big enough to cover the upper spinal cord from the pons down to T5. Normally an FOV of 270- 280mm should be sufficient. The slices should be enough to cover the spinal cord side to side. A saturation band must be placed over the neck in front of the oesophagus in the sagittal plane to avoid swallowing artefacts. The phase direction should be head to foot to avoid motion artefacts from the neck.

Parameters
TR 400-600 | TE 15-25 | SLICE 2MM | FLIP 150 | PHASE H>F | MATRIX 320X320 | FOV 270-280 | GAP 10% | NEX(AVRAGE) 4 |
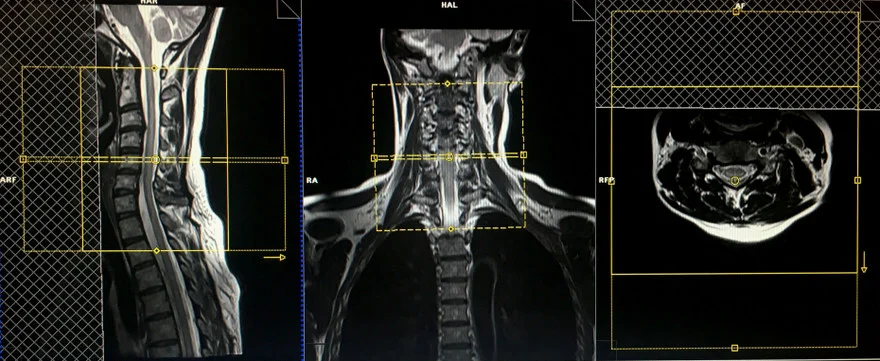
T2 TSE Axial block 3mm 150- 160 FOV
Parameters
TR 3000-4000 | TE 100-120 | SLICE 3 MM | FLIP 130-150 | PHASE A>P | MATRIX 256X256 | FOV 150-160 | GAP 10% | NEX(AVRAGE) 4 |
T1 TSE Axial block 3mm 150- 160 FOV
Plan the axial slices on the sagittal plane, angle the position block perpendicular to the spinal cord. An appropriate angle must be given in the coronal plane on a tilted or scoliotic spine, angling parallel to the intervertebral disc spaces. Slices must be sufficient to cover the area of pathology or cervical cord. In the sagittal plane a saturation band must be placed over the neck in front of the oesophagus to avoid swallowing artefacts.
Parameters
TR 400-600 | TE 15-25 | SLICE 3 MM | FLIP 90 | PHASE A>P | MATRIX 256X256 | FOV 150-160 | GAP 10% | NEX(AVRAGE) 4 |
Next, move the table inward towards the magnet by 250-300mm depending on the patient’s height. Modern scanners provide an auto-table move option which allows the user to plan an isocentered localiser in the lower spine without losing the upper spine localisers. If this options are not available in your scanner please re-enter the patient for the lower cord.
localiser thoraco lumbar spine
A three plane localiser must be taken in the beginning to localise and plan the sequences. Localisers are normally less than 25 seconds long and are T1 weighted low resolution scans.
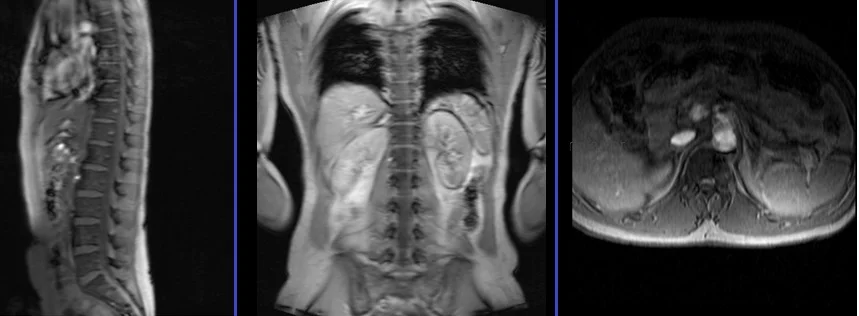
T2 tse sagittal 2mm 270-280 FOV or Isotropic 3D T2 SPACE .9mm
Plan the sagittal slices on the coronal plane, angle the position block parallel to spinal cord. Check the positioning block in the other two planes. An appropriate angle must be given in the axial plane on a tilted patient, this should be parallel to the imaginary line running through the centre of the vertebral body and the spinous process. Check the position block in the sagittal plane where the FOV must be big enough to cover the lower spinal cord from T4 down to L3. Normally an FOV of 270- 280mm should be sufficient. The slices should be enough to cover the spinal cord side to side. In the sagittal plane a saturation band must be placed over the abdomen in front of the aorta to avoid peristalsis and breathing artefacts. Phase direction should be head to foot to avoid motion artefacts from the abdomen.

Parameters
TR 3000-4000 | TE 100-120 | SLICE 2 MM | FLIP 130-150 | PHASE H>F | MATRIX 320X320 | FOV 270-280 | GAP 10% | NEX(AVRAGE) 4 |
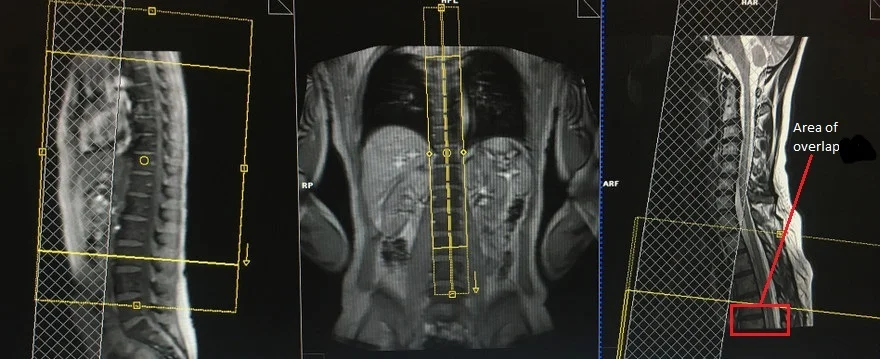
It is important to have some overlap of the spinal cord to avoid missed anatomy. For example, if the upper sagittal sequences cover the spinal cord from the pons down to T5 then the lower sagittal sequences must cover the spinal cord from T4 down to L3.
T1 tse sagittal 2mm 270-280 FOV or Isotropic 3D T1 .9mm
Plan the sagittal slices on the coronal plane, angle the position block parallel to spinal cord. Check the positioning block in the other two planes. An appropriate angle must be given in the axial plane on a tilted patient, this should be parallel to the imaginary line running through the centre of the vertebral body and the spinous process. Check the position block in the sagittal plane where the FOV must be big enough to cover the lower spinal cord from T4 down to L3. Normally an FOV of 270- 280mm should be sufficient. The slices should be enough to cover the spinal cord side to side. In the sagittal plane a saturation band must be placed over the abdomen in front of the aorta to avoid peristalsis and breathing artefacts. Phase direction should be head to foot to avoid motion artefacts from the abdomen.

Parameters
TR 400-600 | TE 15-25 | SLICE 2 MM | FLIP 150 | PHASE H>F | MATRIX 320X320 | FOV 270-280 | GAP 10% | NEX(AVRAGE) 4 |
T2 TSE Axial block 3mm 150- 160 FOV
Axial scans are only performed over spinal cord pathologies e.g. MS lesions or a syrinx. Axial scanning can be avoided in the lower sagittal sequences if no pathologies are identified.
Plan the axial slices on the sagittal plane, angle the position block perpendicular to the spinal cord. An appropriate angle must be given in the coronal plane on a tilted or scoliotic spine, angling parallel to the intervertebral disc spaces. Slices must be sufficient to cover the area of pathology. In the sagittal plane a saturation band must be placed over the abdomen in front of the aorta to avoid peristalsis and breathing artefacts. Phase direction should be head to foot to avoid further motion artefacts from the abdomen.

Parameters
TR 3000-4000 | TE 100-120 | SLICE 3 MM | FLIP 130-150 | PHASE A>P | MATRIX 256X256 | FOV 150-160 | GAP 10% | NEX(AVRAGE) 4 |
T1 TSE Axial block 3mm 150- 160 FOV
Plan the axial slices on the sagittal plane, angle the position block perpendicular to the spinal cord. An appropriate angle must be given in the coronal plane on a tilted or scoliotic spine, angling parallel to the intervertebral disc spaces. Slices must be sufficient to cover the area of pathology. In the sagittal plane a saturation band must be placed over the abdomen in front of the aorta to avoid peristalsis and breathing artefacts. Phase direction should be head to foot to avoid further motion artefacts from the abdomen.
Parameters
TR 400-600 | TE 15-25 | SLICE 3 MM | FLIP 90 | PHASE A>P | MATRIX 256X256 | FOV 150-160 | GAP 10% | NEX(AVRAGE) 4 |
CLICK THE SEQUENCES BELOW TO CHECK THE SCANS
- localize C-T spine_3plane1
- T2_sagittal_large FOV2
- T2_sagittal_2mm_SFOV3
- T1_sagittal_2mm_SFOV4
- T2_axial_3mm_SFOV5
- T1_axial_3mm_SFOV6
- localize T-L spine_3plane7
- T2_sagittal_2mm_SFOV8
- T1_sagittal_2mm_SFOV9
- T2_axial_3mm_SFOV10
- T1_axial_3mm_SFOV11
-
CONTRAST ENHANCEMENT

- T1_sagittal_fat sat_post gd_2mm12
- T1_axial_fat sat_post gd_2mmL13
- T1_sagittal_fat sat_post gd_2mm14
- T1_axial_fat sat_post gd_2mm15