Collagen VI-Related Myopathies MRI
Collagen VI-related myopathies are a group of genetic muscle disorders caused by mutations in the genes responsible for producing collagen VI, a crucial protein for muscle and connective tissue structure and function. These myopathies include conditions such as Bethlem myopathy and Ullrich congenital muscular dystrophy.
Cause
Collagen VI-related myopathies are primarily caused by mutations in the COL6A1, COL6A2, and COL6A3 genes. These genes provide instructions for making the collagen VI protein, which is vital for maintaining the integrity and stability of muscle cells. Mutations in these genes lead to the production of defective collagen VI or reduced amounts of it, resulting in muscle weakness and other associated symptoms.
Symptoms
The symptoms of Collagen VI-related myopathies can appear at birth or develop in early childhood, and in milder cases, during adolescence or adulthood. Common symptoms include:
- Muscle weakness, particularly in the shoulders, upper arms, hips, and thighs.
- Joint hypermobility in the hands and feet, contrasted with joint contractures (stiffening or tightening) that may develop in the elbows, ankles, and spine.
- Respiratory difficulties due to weakness of the respiratory muscles.
- Skin abnormalities such as keloid scar formation and hyperkeratosis (thickening of the skin).
- Easy bruising.
Patients with a more severe form, like Ullrich congenital muscular dystrophy, may exhibit pronounced muscle weakness and joint issues from birth. Those with milder forms, such as Bethlem myopathy, may have a slower progression of muscle weakness and may achieve normal motor milestones.
Diagnosis
Diagnosing Collagen VI-related myopathies typically involves a combination of clinical examination, family history, and several tests:
- Genetic testing to identify mutations in COL6A1, COL6A2, or COL6A3.
- Muscle biopsy to analyze muscle tissue structure and the presence of collagen VI.
- Imaging studies like MRI to assess muscle quality and involvement.
- Electromyography (EMG) to measure the electrical activity of muscles.
- Pulmonary function tests to evaluate respiratory capability.
Treatment
There is currently no cure for Collagen VI-related myopathies, and treatment focuses on managing symptoms and improving quality of life:
- Physiotherapy to maintain muscle strength and joint range of motion.
- Orthopedic interventions to manage joint contractures and scoliosis.
- Respiratory support, which may include non-invasive ventilation, especially during sleep.
- Regular monitoring by a multidisciplinary team including neurologists, orthopedists, and pulmonologists.
- Genetic counseling to provide families with information on the inheritance pattern and implications for future pregnancies.
MRI Appearance of Collagen VI-Related Myopathies
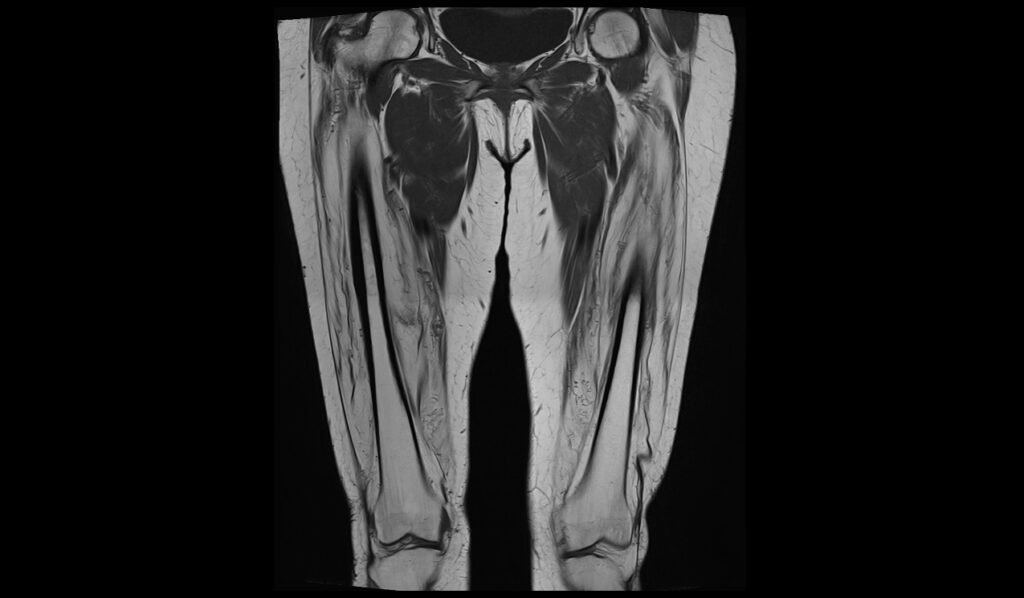
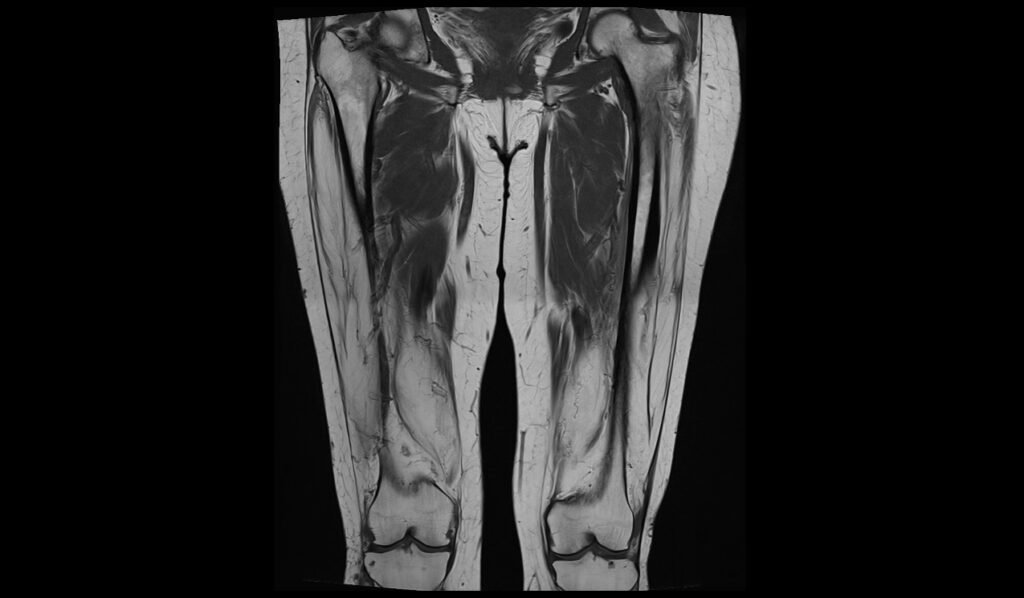
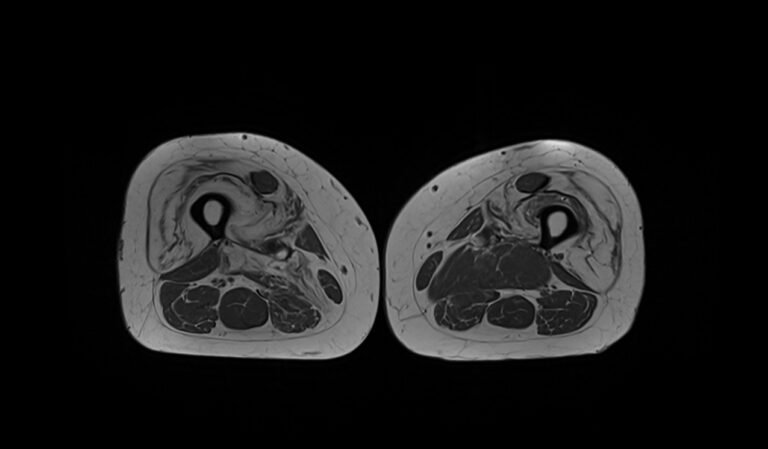
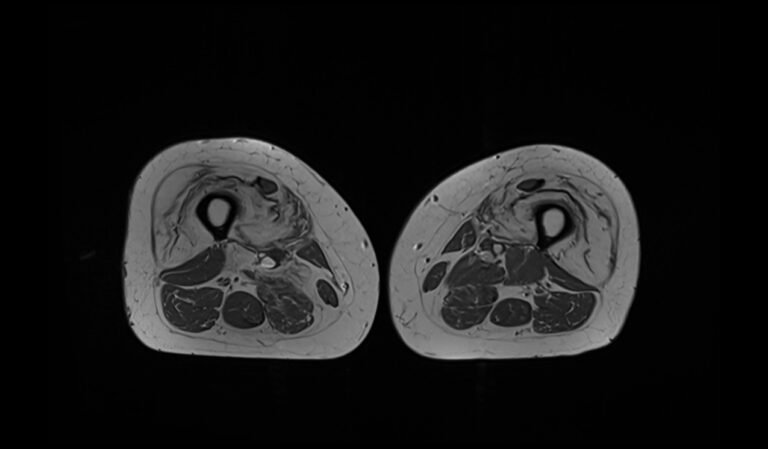
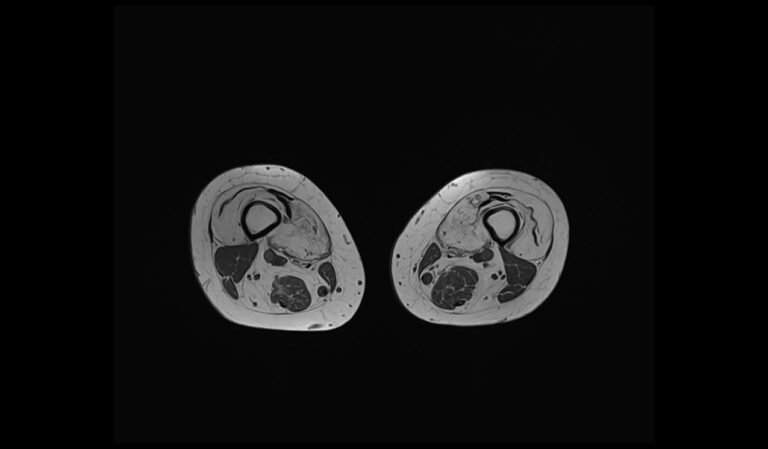
MRI T1 Appearance of Collagen VI-Related Myopathies
In T1-weighted MRI images, Collagen VI-related myopathies typically present with characteristic patterns of muscle involvement. The muscles may exhibit a mixture of normal and abnormal signals, with areas of fatty infiltration appearing hyperintense (bright). This fatty replacement often affects specific muscle groups, such as the quadriceps, hamstrings, and calf muscles, leading to a patchy or lobulated appearance. Additionally, the overall muscle volume may be reduced, and there may be evidence of muscle atrophy. These T1-weighted images are crucial for identifying the extent of chronic changes and distinguishing between affected and unaffected muscles in patients with Collagen VI-related myopathies.
MRI T2 Appearance of Collagen VI-Related Myopathies
On T2-weighted MRI images, Collagen VI-related myopathies typically show areas of increased signal intensity due to edema and inflammation within the muscles. These hyperintense (bright) regions highlight the active disease process, including muscle fiber necrosis and regeneration. The T2 images may also reveal muscle swelling and variations in muscle texture, indicative of ongoing muscle damage and repair. The presence of hyperintense signals in specific muscle groups can help in diagnosing the myopathy and assessing the severity of the condition. These T2-weighted images are essential for evaluating the inflammatory aspects of the disease and monitoring the response to therapy.
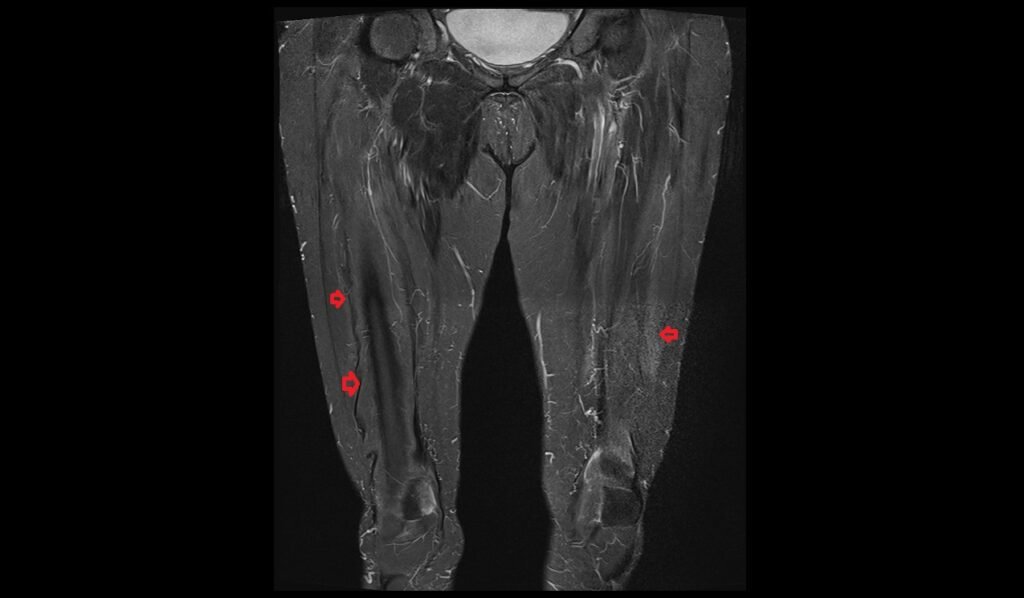
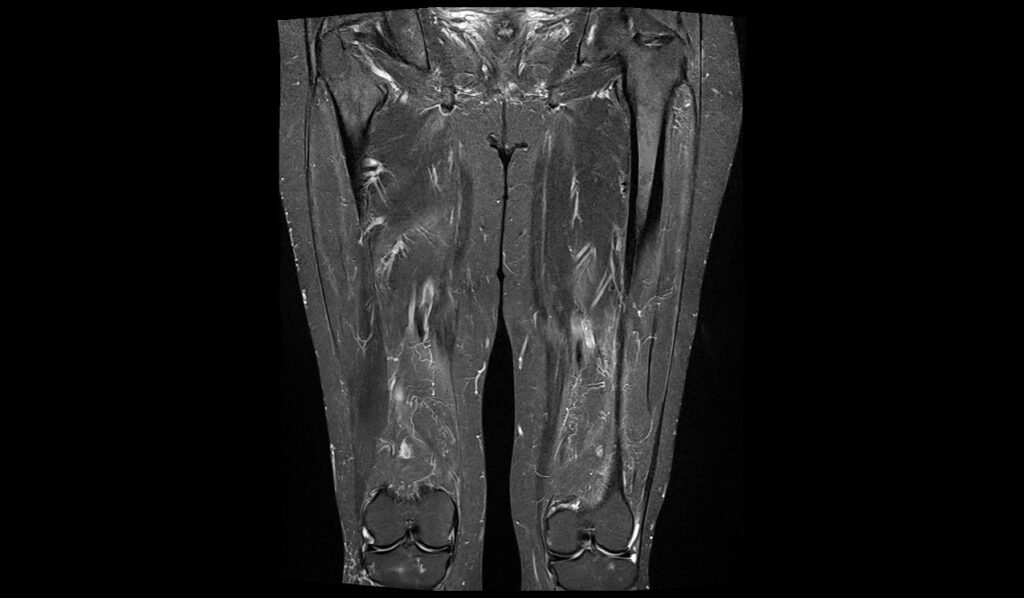
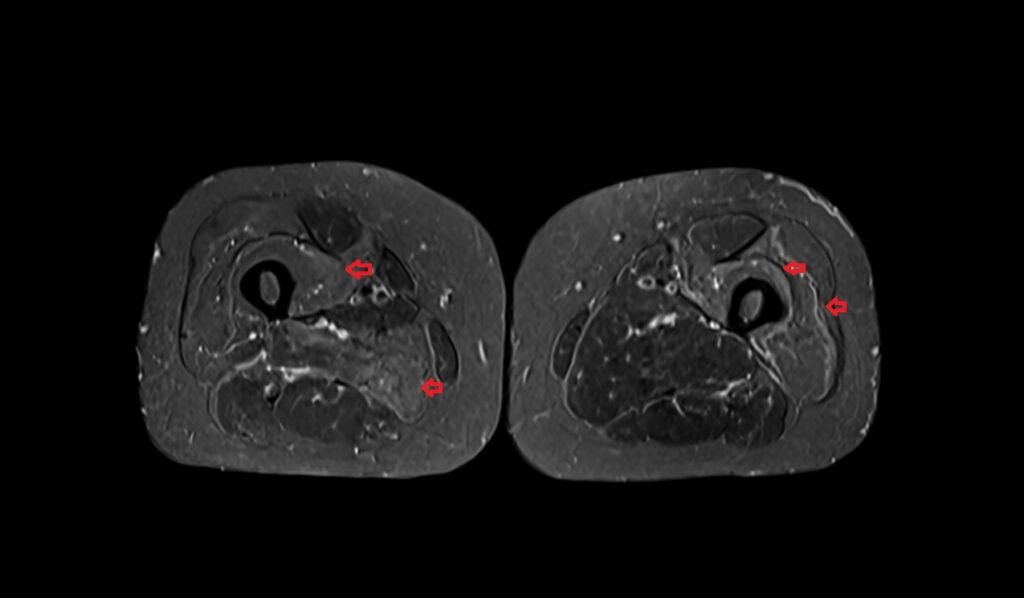
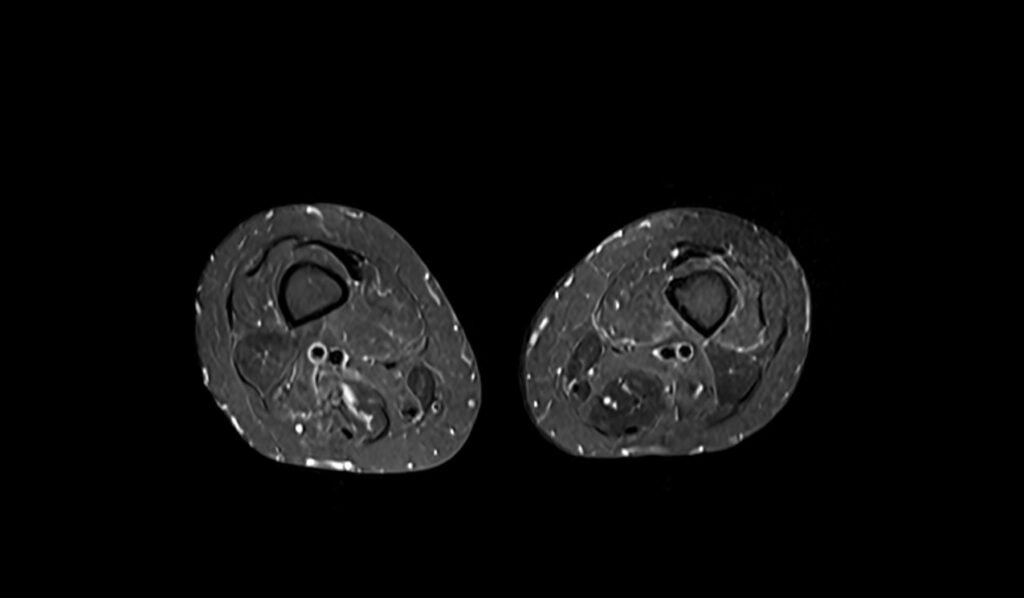
MRI STIR Appearance of Collagen VI-Related Myopathies
Short Tau Inversion Recovery (STIR) MRI sequences are highly sensitive to detecting muscle edema and inflammation, making them particularly useful for assessing Collagen VI-related myopathies. In STIR images, affected muscles often appear hyperintense (bright) due to the presence of increased water content associated with edema. This sequence can highlight areas of active disease, distinguishing between inflammatory and non-inflammatory muscle changes. The high sensitivity of STIR imaging to fluid changes provides valuable information about the extent and activity of the myopathy, aiding in the diagnosis and management of patients with Collagen VI-related myopathies.
MRI STIR Appearance of Collagen VI-Related Myopathies


MRI T1 Appearance of Collagen VI-Related Myopathies


STIR axial image of thigh shows Infectious Myositis

T1 TSE axial image of thigh shows Infectious Myositis
References
- Kwong, A. K. Y., Zhang, Y., Ho, R. S. L., Bönnemann, C. G., Javed, A., & Chan, S. H. S. (2023). Collagen VI-related myopathies: Clinical variability, phenotype-genotype correlation and exploratory transcriptome study. Neuromuscular Disorders, 33(5), 371-381.
- Bönnemann, C. G. (2011). The collagen VI-related myopathies: Muscle meets its matrix. Nature Reviews Neurology, 7(7), 379–390. https://doi.org/10.1038/nrneurol.2011.81