Clival Chordoma MRI
Clival chordomas are rare, slow-growing malignant tumors that occur at the base of the skull in a region called the clivus. They originate from remnants of the notochord, an embryonic structure that contributes to the development of the spinal column. These tumors account for a small percentage of all skull base tumors but can cause significant morbidity due to their location near critical neurological structures.
Causes
The exact cause of clival chordomas is not well understood. They arise from notochordal remnants, but why these remnants transform into tumors is unclear. Potential factors might include genetic mutations or hereditary predispositions, but more research is needed to pinpoint specific causes.
Symptoms
Symptoms of clival chordomas often develop gradually and can vary widely depending on the size and exact location of the tumor. Common symptoms include:
- Headache: Often a persistent and severe headache, typically in the back of the head.
- Double Vision (Diplopia): Due to the involvement of cranial nerves controlling eye movement.
- Hearing Loss: If the tumor affects the auditory pathways.
- Facial Pain or Numbness: Resulting from compression of cranial nerves.
- Difficulty Swallowing (Dysphagia): If the tumor compresses structures involved in swallowing.
- Horner’s Syndrome: A combination of drooping eyelid (ptosis), pupil constriction (miosis), and lack of sweating (anhidrosis) on one side of the face.
Diagnosis
Diagnosing clival chordomas typically involves a combination of imaging studies and biopsy:
- Magnetic Resonance Imaging (MRI): Provides detailed images of the tumor and its relationship with surrounding structures. It is the preferred imaging modality.
- Computed Tomography (CT) Scan: Useful for evaluating bone involvement and destruction.
- Biopsy: A sample of the tumor tissue is obtained, usually through a surgical procedure, and examined under a microscope to confirm the diagnosis.
Treatment
Treatment of clival chordomas often requires a multidisciplinary approach, including surgery, radiation therapy, and sometimes targeted therapies.
- Surgery: The primary treatment is surgical resection. The goal is to remove as much of the tumor as possible while preserving neurological function. Due to the tumor’s location near critical structures, complete resection can be challenging.
- Radiation Therapy: Postoperative radiation therapy, such as proton beam therapy, is commonly used to target residual tumor cells. Proton therapy is preferred due to its precision and ability to spare surrounding healthy tissue.
- Targeted Therapy and Chemotherapy: These are less commonly used but may be considered in cases where surgery and radiation are not fully effective. Research is ongoing into specific molecular targets for chordomas.
MRI appearance of Clival Chordoma
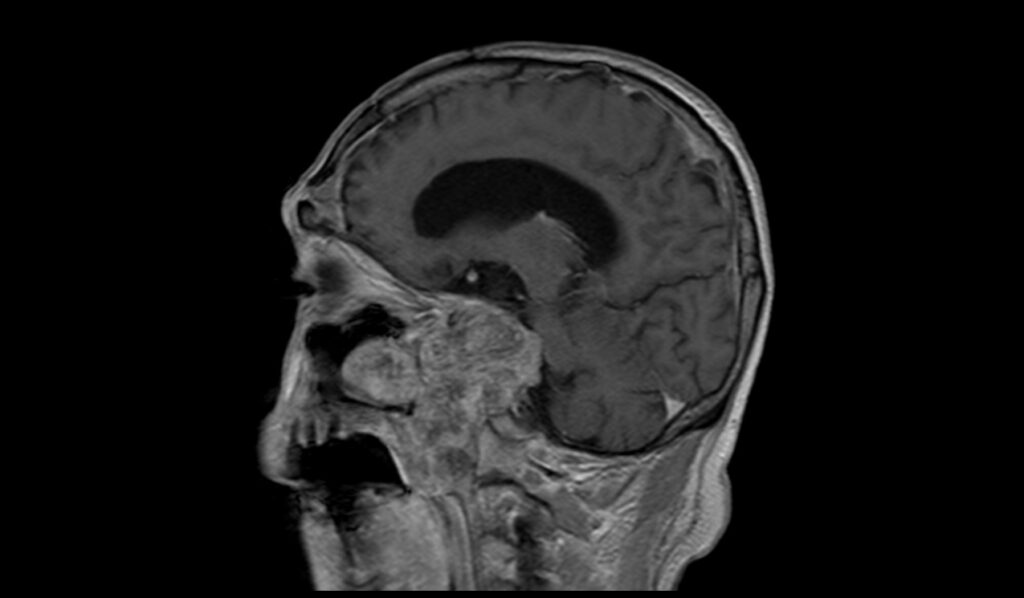
MRI T1 Appearance of Clival Chordoma
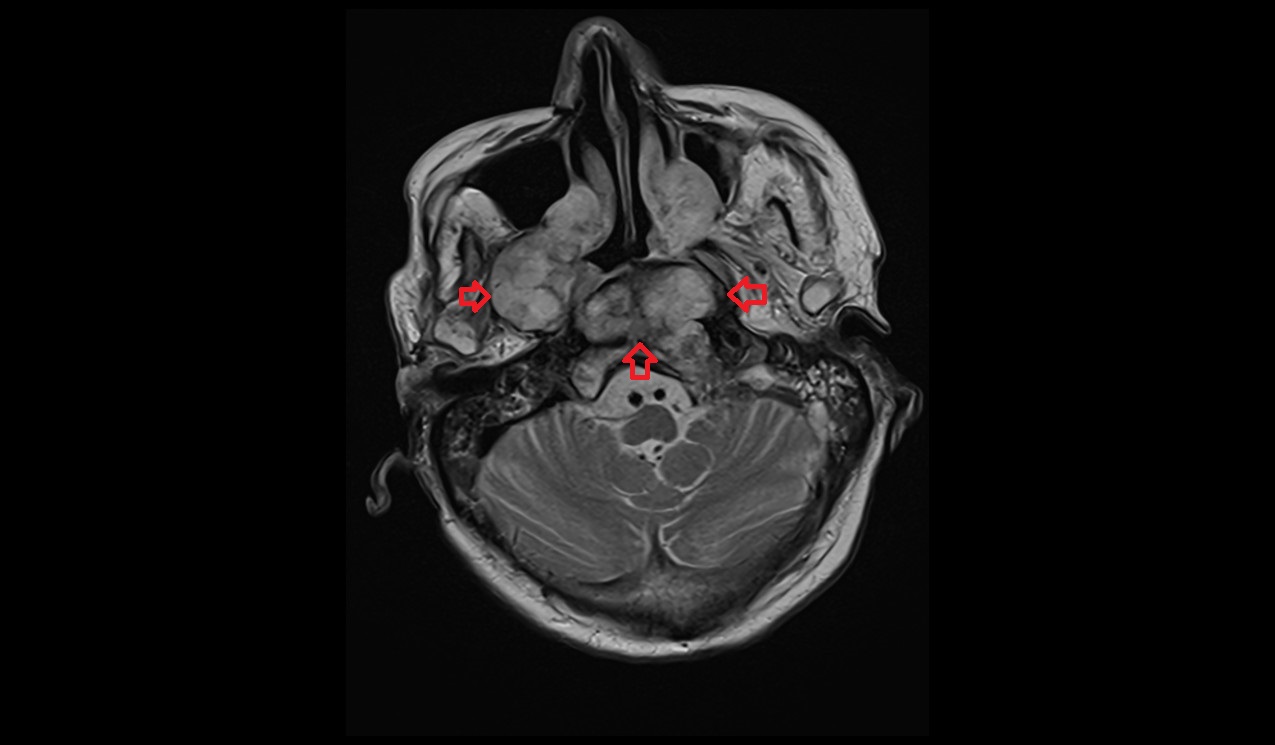
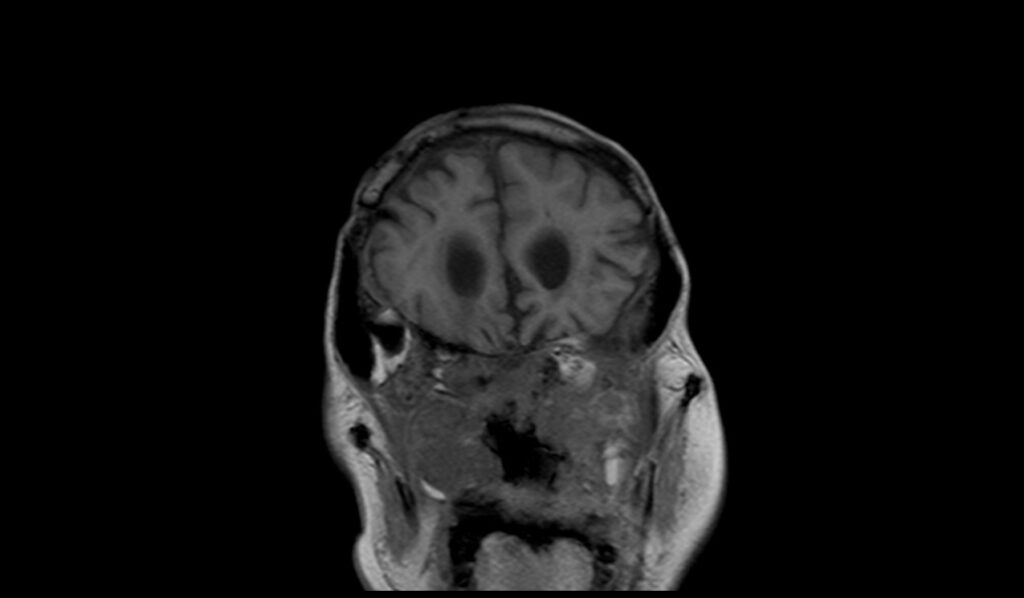
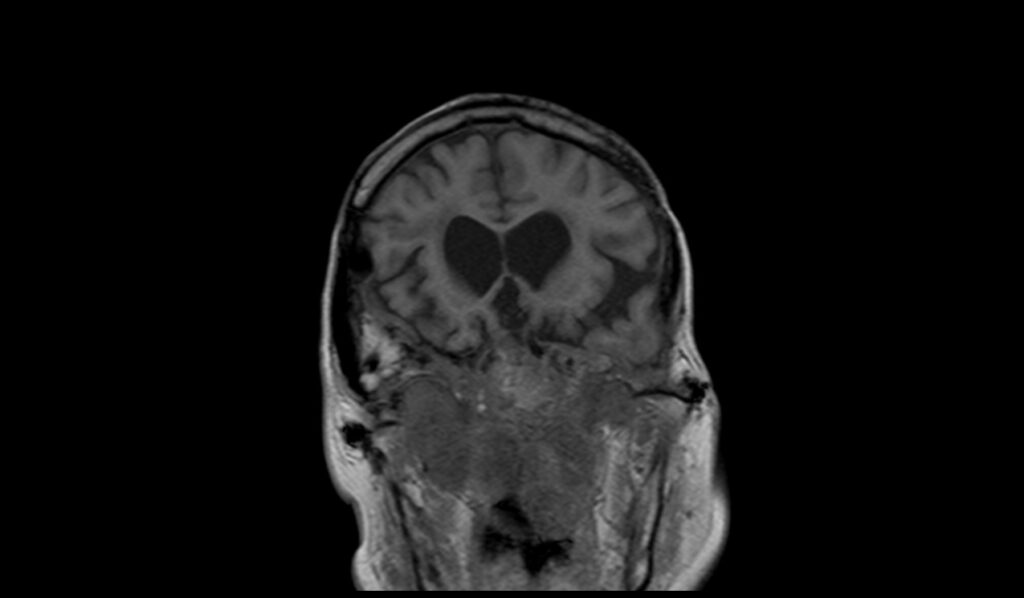
On T1-weighted MRI images, clival chordomas typically appear as hypointense (dark) relative to the surrounding brain tissue. This low signal intensity helps distinguish the chordoma from the adjacent structures. However, the presence of hemorrhage within the tumor can cause areas of hyperintensity (bright signal), leading to a heterogeneous appearance. These variations in signal intensity on T1-weighted images provide crucial information about the composition and extent of the chordoma.
MRI T2 Appearance of Clival Chordoma
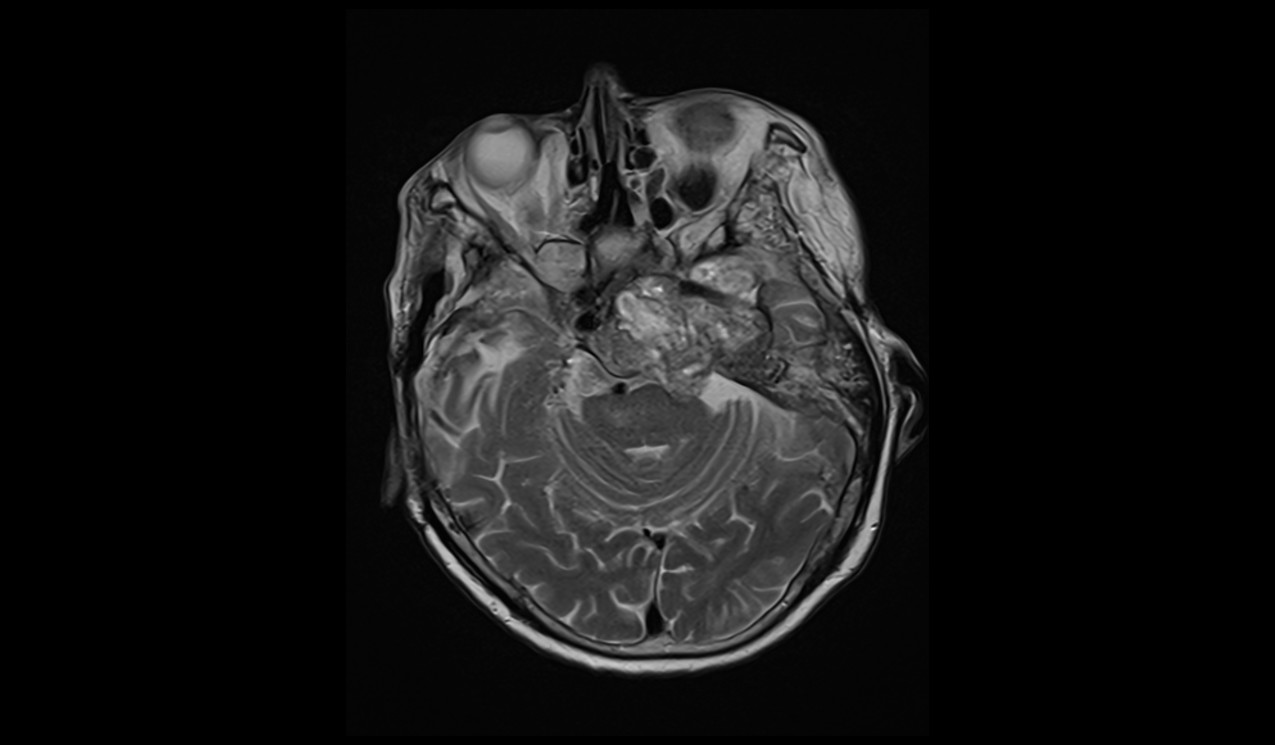
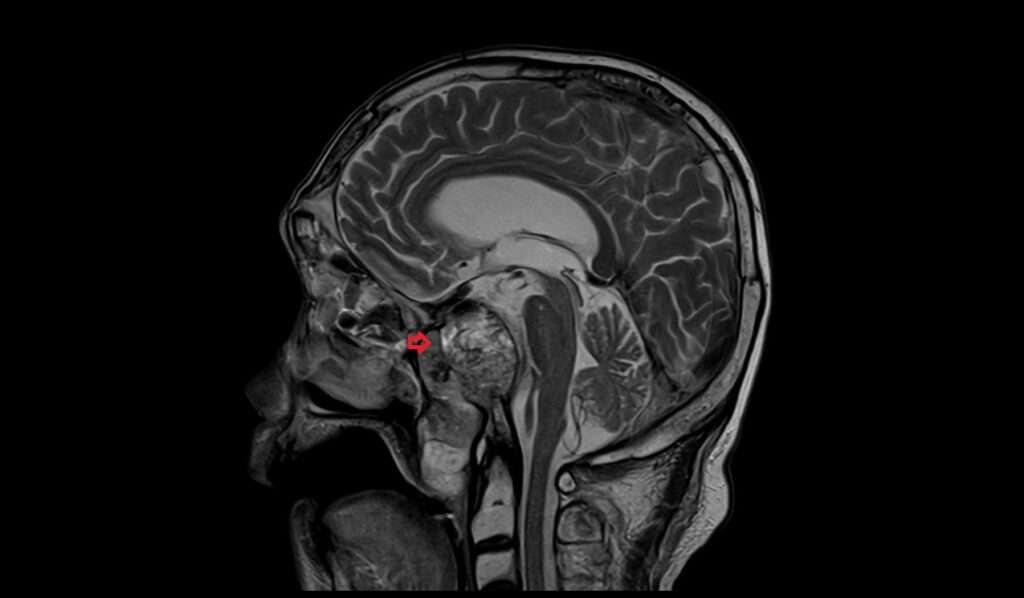
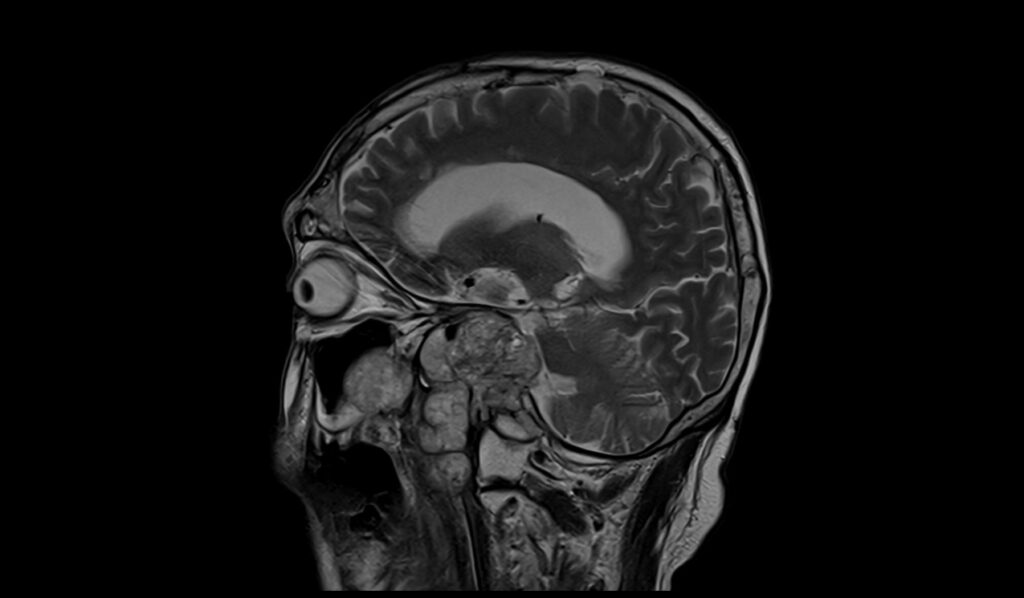
T2-weighted MRI images of clival chordomas generally show hyperintense (bright) signal intensity, making the tumor stand out against the normal brain tissue. The high water content of the chordoma contributes to this bright signal. However, the presence of hemorrhage within the tumor can result in mixed signal intensity, with areas of hypointensity (dark signal) corresponding to the hemorrhagic regions. This heterogeneous appearance on T2 images can provide valuable information about the tumor’s internal structure and potential complications.
MRI FLAIR Appearance of Clival Chordoma
On FLAIR (Fluid-Attenuated Inversion Recovery) MRI images, clival chordomas typically appear as hyperintense (bright) areas. FLAIR imaging suppresses the signal from cerebrospinal fluid, enhancing the visibility of lesions and making the chordoma more conspicuous. The high signal intensity on FLAIR images indicates the presence of a solid mass, which can be useful in differentiating the chordoma from other cystic lesions in the same region.
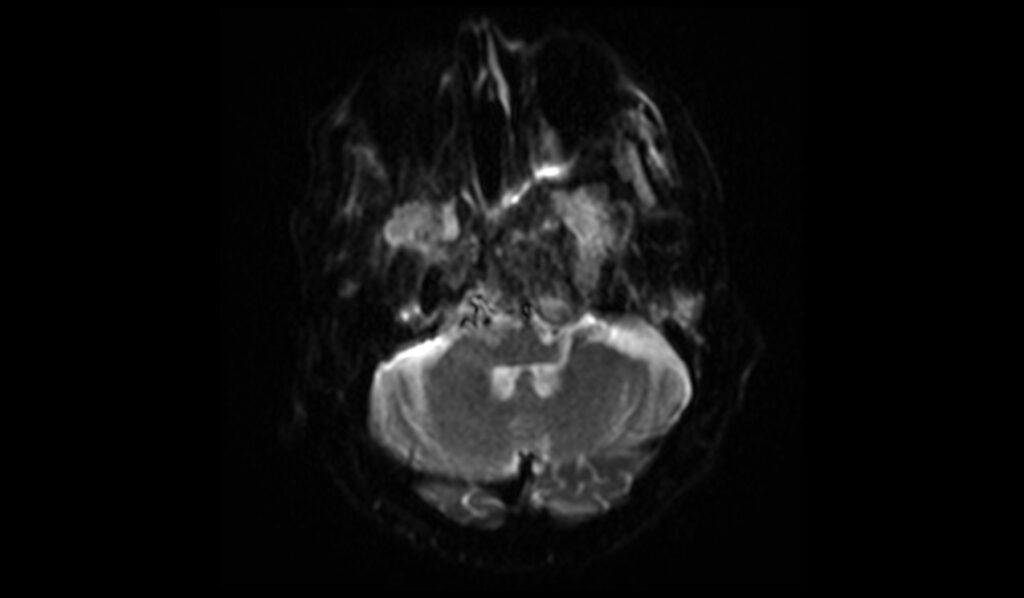
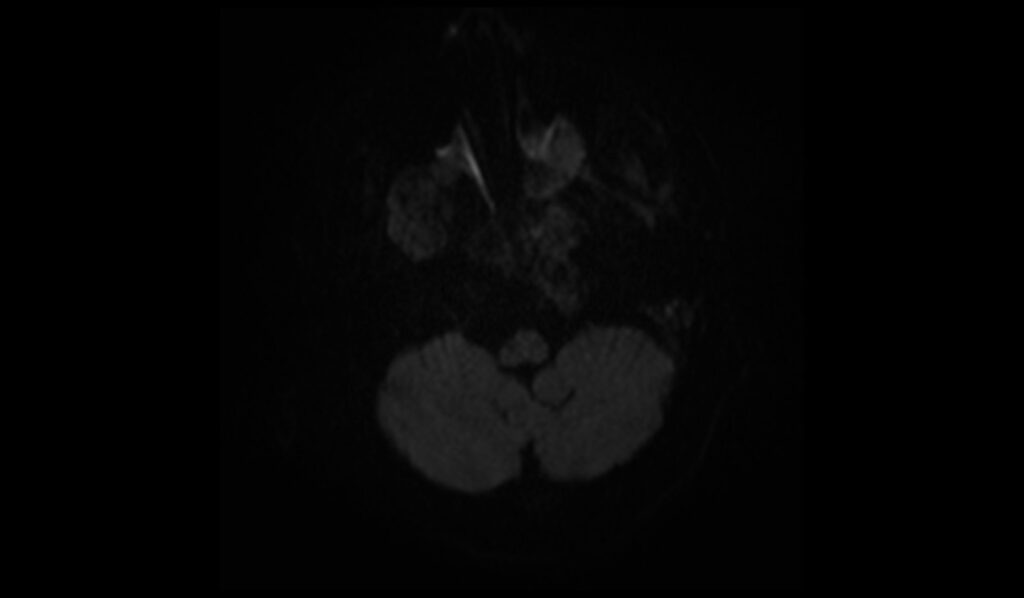
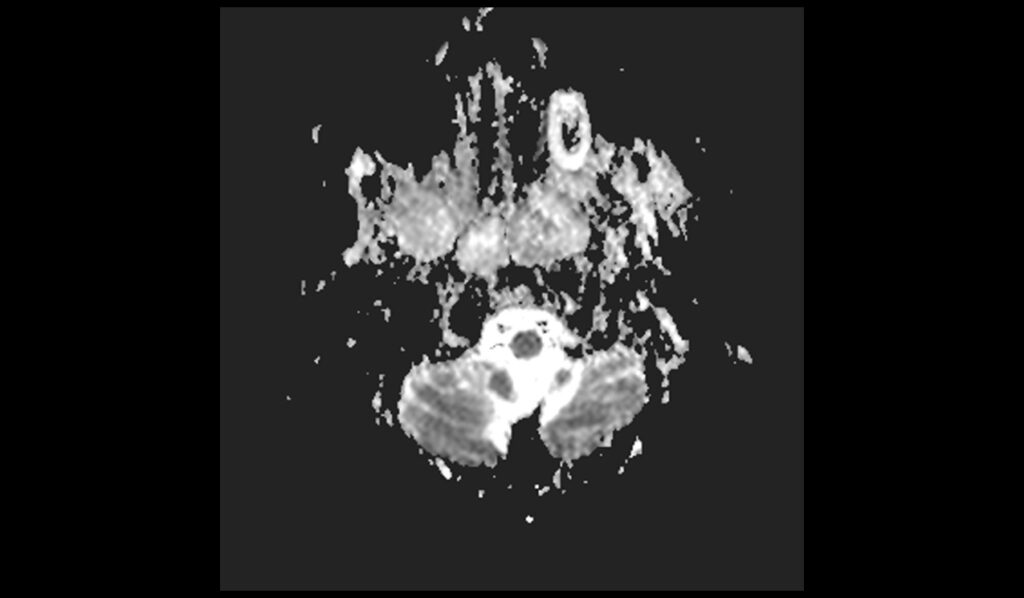
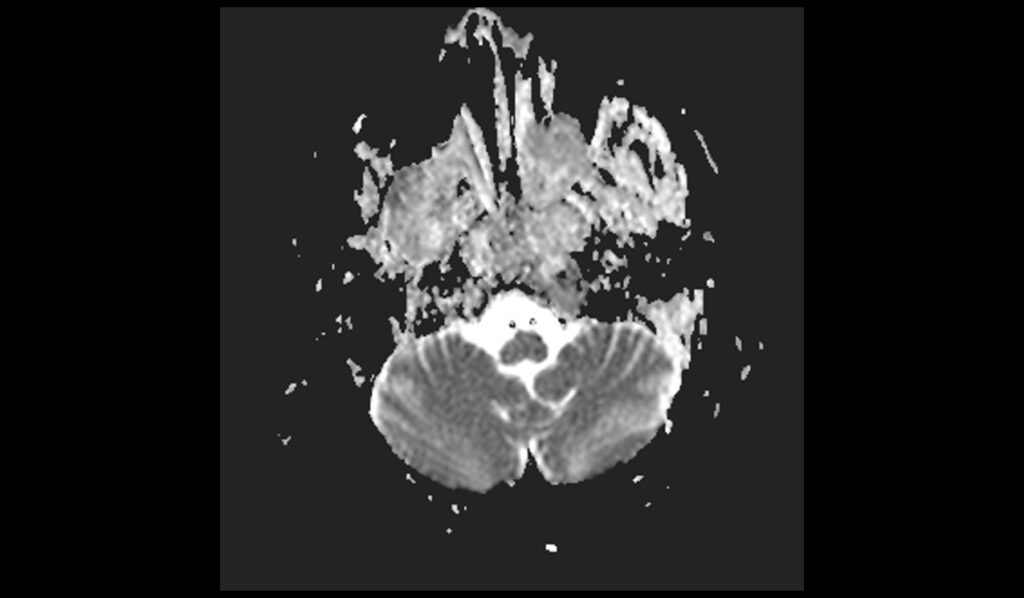
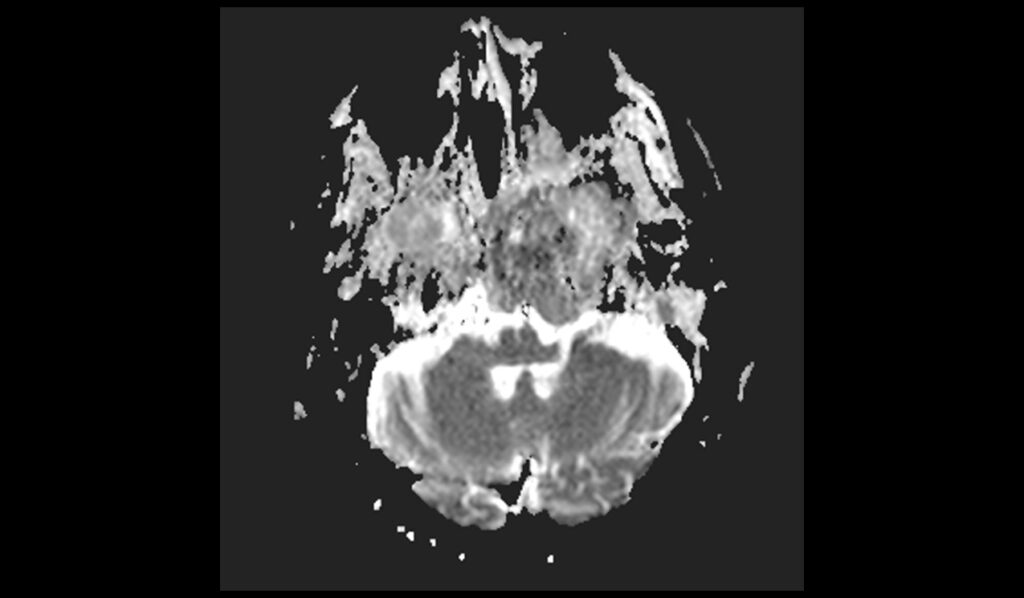
MRI DWI and ADC Appearance of Clival Chordoma
Diffusion-weighted imaging (DWI) and apparent diffusion coefficient (ADC) maps are essential for evaluating the cellularity of clival chordomas. On DWI, chordomas usually show low to intermediate signal intensity due to their relatively low cellularity compared to high-grade tumors. However, in cases of hemorrhage within the tumor, there can be mixed signal intensity, with areas of high signal corresponding to restricted diffusion. On ADC maps, chordomas typically exhibit high signal intensity, reflecting the high diffusivity of water molecules within the tumor. This combination of DWI and ADC characteristics helps in assessing the nature and aggressiveness of the chordoma.
MRI T1 Post-Contrast Appearance of Clival Chordoma
Following the administration of contrast material, T1-weighted post-contrast MRI images of clival chordomas typically show heterogeneous enhancement. This enhancement pattern is due to the presence of both solid and cystic components within the tumor. The solid parts of the chordoma enhance more intensely, while the cystic or necrotic areas may show little to no enhancement. This post-contrast imaging is crucial for delineating the tumor boundaries, evaluating its extent, and planning surgical or therapeutic interventions.
T2 axial image shows clival chordoma
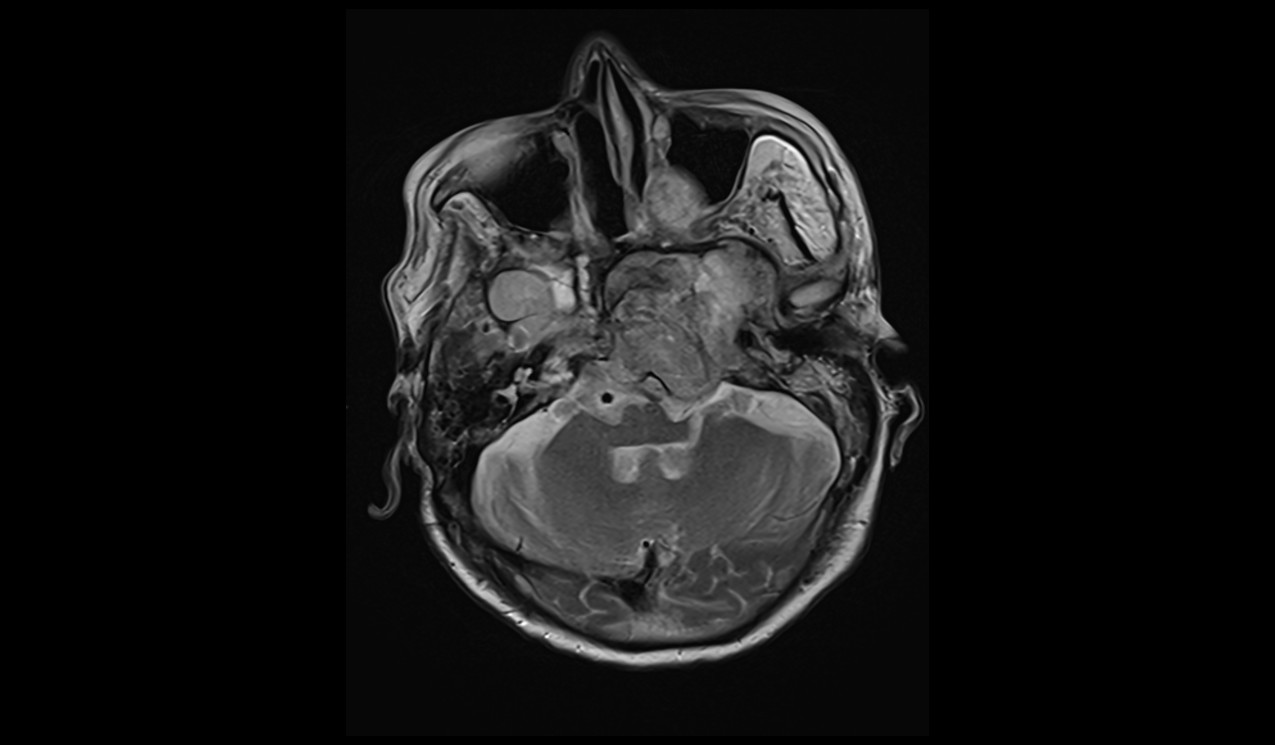
FLAIR axial image shows clival chordoma



T1 coronal images shows clival chordoma

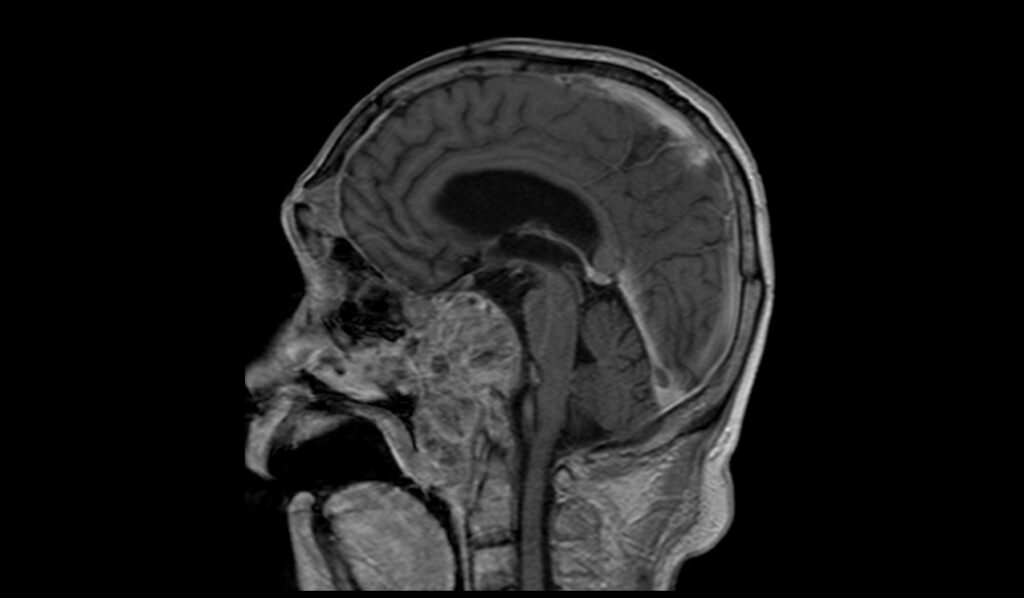
T2 sagittal images shows clival chordoma
DWI b0 images shows clival chordoma
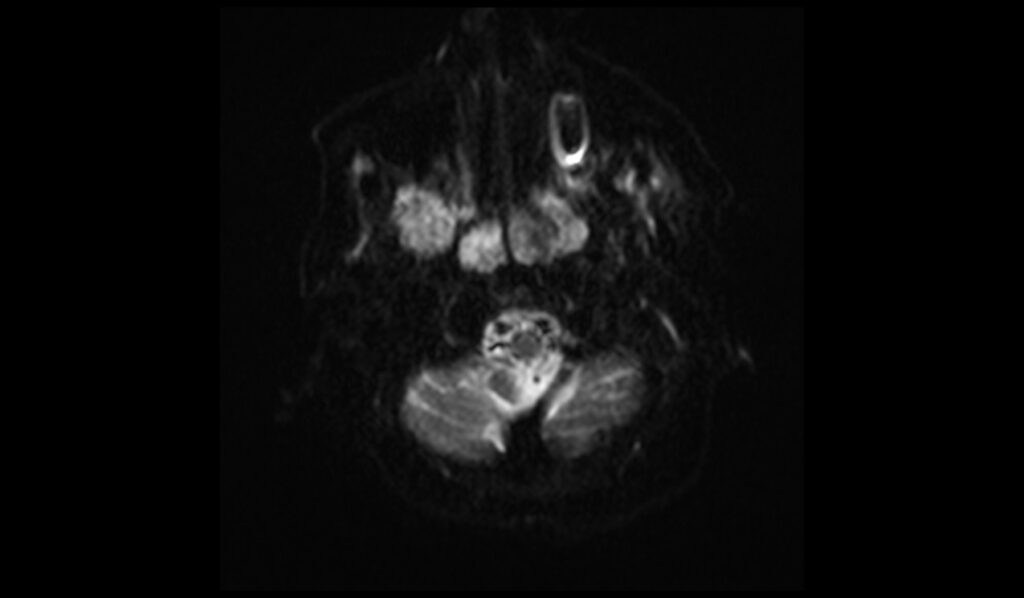
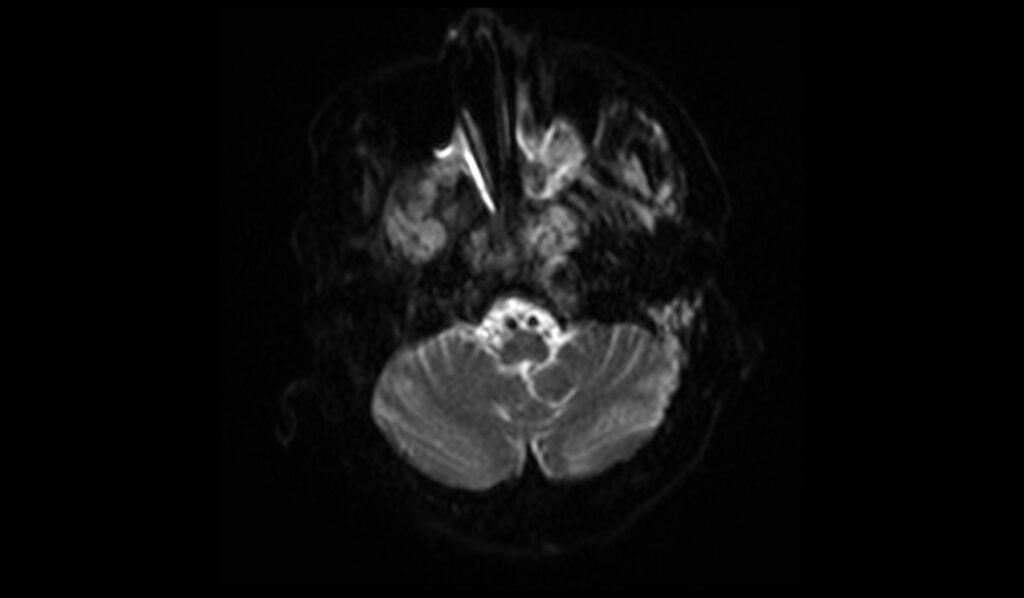
DWI b1000 images shows clival chordoma
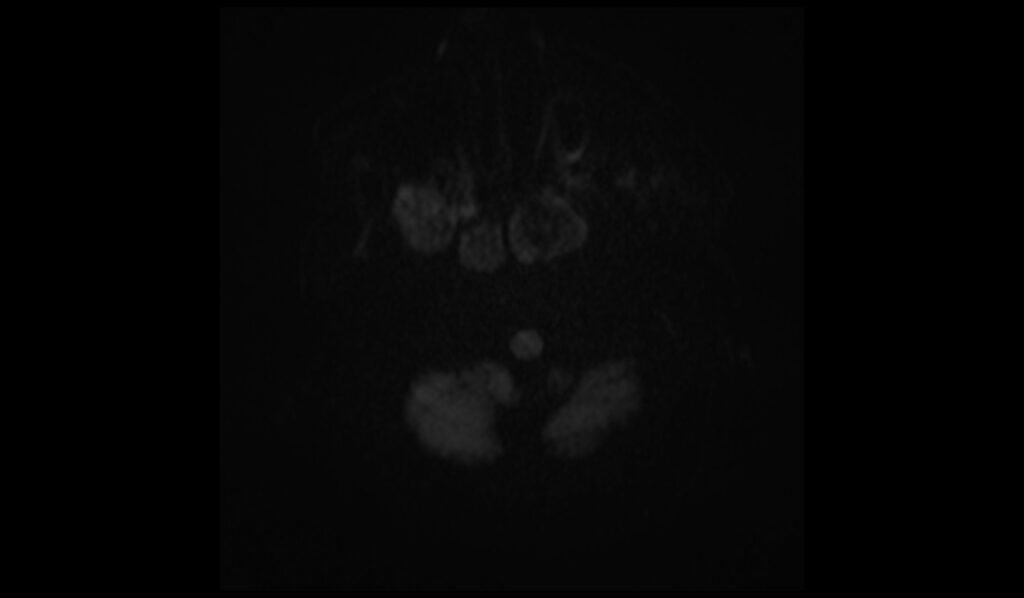

DWI ADC images shows clival chordoma
T1 post contrast axial images shows clival chordoma


T1 post contrast sagittal images shows clival chordoma
T1 post contrast coronal images shows clival chordoma

References
- Guadalupi, P., Gessi, M., Massimi, L., Caldarelli, M., & Gaudino, S. (2022). A cystic clival chordoma with CT and MRI unconventional appearances. Indian Journal of Radiology and Imaging, 32(1), 127-131. doi: 10.1055/s-0041-1741044. PMID: 35722639. PMCID: PMC9200489. Published online 2022 Feb 28. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9200489/
- Yeom, K. W., Lober, R. M., Mobley, B. C., Harsh, G., Vogel, H., Allagio, R., Pearson, M., Edwards, M. S. B., & Fischbein, N. J. (2013). Diffusion-weighted MRI: Distinction of skull base chordoma from chondrosarcoma. American Journal of Neuroradiology, 34(5), 1056-1061. https://doi.org/10.3174/ajnr.A3333
- Machida, T., Aoki, S., Sasaki, Y., & Iio, M. (1986). Magnetic resonance imaging of clival chordomas. Acta Radiologica Supplementum, 369, 167-169. https://pubmed.ncbi.nlm.nih.gov/2980441/
- Zribi A, Ben Nasr S, Khemir A, Gargouri F, Ben Abdallah I, Msakni I, Fendri S, Balti M, Laabidi B, Haddaoui A. Clival chordoma in a young male patient: a case report. Pan African Medical Journal. 2020;37:59. doi: 10.11604/pamj.2020.37.59.24836. Available from: https://www.panafrican-med-journal.com/content/article/37/59/full