ALPSA Lesion MRI
Causes
ALPSA lesions are most commonly caused by a traumatic event, typically involving an anterior dislocation of the shoulder. This can occur during high-impact sports, falls, or direct blows to the shoulder that forcibly push the arm backward and outward.
Symptoms
Symptoms of an ALPSA lesion can vary but generally include:
- Shoulder pain, particularly during movement
- A feeling of instability or looseness in the shoulder
- Recurrent shoulder dislocations or subluxations (partial dislocations)
- Decreased range of motion
- Weakness in the shoulder
- A clicking or popping sensation in the shoulder
Diagnosis
Diagnosing an ALPSA lesion typically involves a combination of patient history, physical examination, and imaging studies:
- Patient History: A detailed account of how the injury occurred and the symptoms experienced.
- Physical Examination: The doctor will assess the shoulder’s range of motion, stability, and look for signs of pain or weakness.
- Imaging Studies:
- X-rays: To rule out fractures and other bony abnormalities.
- Magnetic Resonance Imaging (MRI): The most effective tool for visualizing soft tissue injuries, including the labrum and periosteum.
- MRI Arthrogram: An MRI with a contrast agent injected into the shoulder joint can provide more detailed images of the labrum and surrounding structures.
Treatment
Treatment for an ALPSA lesion can be non-surgical or surgical, depending on the severity of the injury and the patient’s activity level and overall health.
Non-Surgical Treatment:
- Rest: Avoid activities that exacerbate the pain or instability.
- Physical Therapy: Focuses on strengthening the muscles around the shoulder, improving range of motion, and enhancing stability.
- Medications: Nonsteroidal anti-inflammatory drugs (NSAIDs) to manage pain and inflammation.
Surgical Treatment:
- Surgery is often recommended for patients with persistent instability, recurrent dislocations, or significant functional impairment. The main surgical options include:
- Arthroscopic Repair: A minimally invasive procedure where small instruments and a camera are inserted through small incisions to reattach the labrum to the glenoid.
- Open Surgery: In some cases, a more invasive open surgical procedure may be necessary, especially if there are additional complications or significant damage.
MRI Appearance of ALPSA Lesion
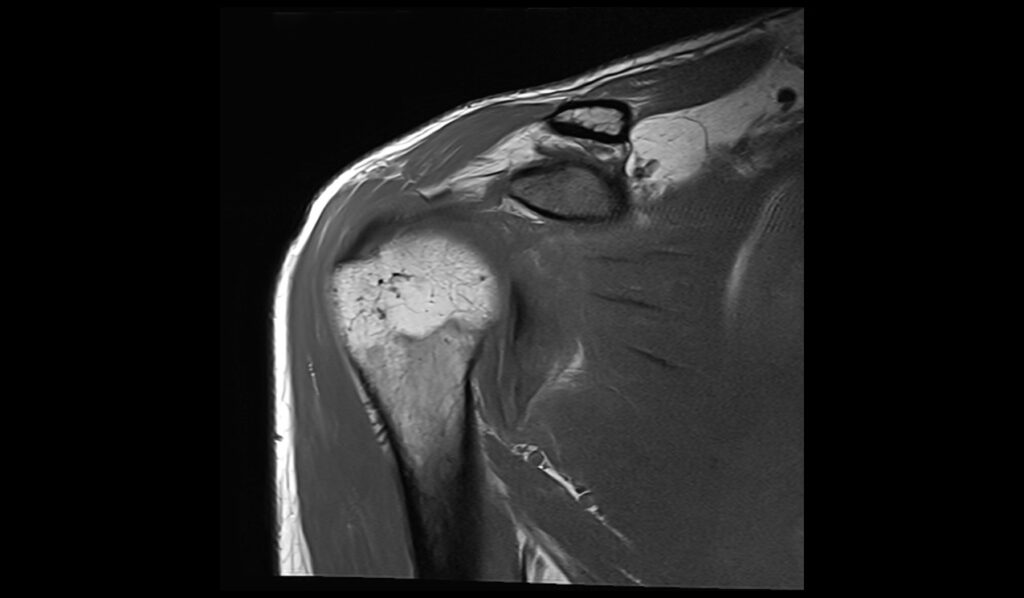
MRI T1 Appearance of ALPSA Lesion
On T1-weighted MRI images, an Anterior Labral Periosteal Sleeve Avulsion (ALPSA) lesion may appear as a discontinuity or irregularity in the normal contour of the anterior labrum. The lesion itself may exhibit an intermediate to low signal intensity compared to the surrounding structures. This imaging sequence is useful for identifying the anatomical details and any associated bony injuries or alterations in the glenoid rim, which can appear as subtle signal changes or bone marrow edema. The T1 sequence helps in assessing the integrity of the soft tissues and the overall anatomy of the shoulder joint.
MRI T2 Appearance of ALPSA Lesion
T2-weighted MRI images provide excellent contrast for visualizing fluid and edema, which are often present in the case of an ALPSA lesion. On T2 images, the lesion typically appears as a hyperintense (bright) signal due to the presence of joint fluid or inflammation around the torn labrum. The retracted labral tissue and any associated capsuloperiosteal stripping from the glenoid may be clearly delineated. This sequence is particularly useful for identifying the extent of soft tissue injury and for detecting associated joint effusion or synovitis.
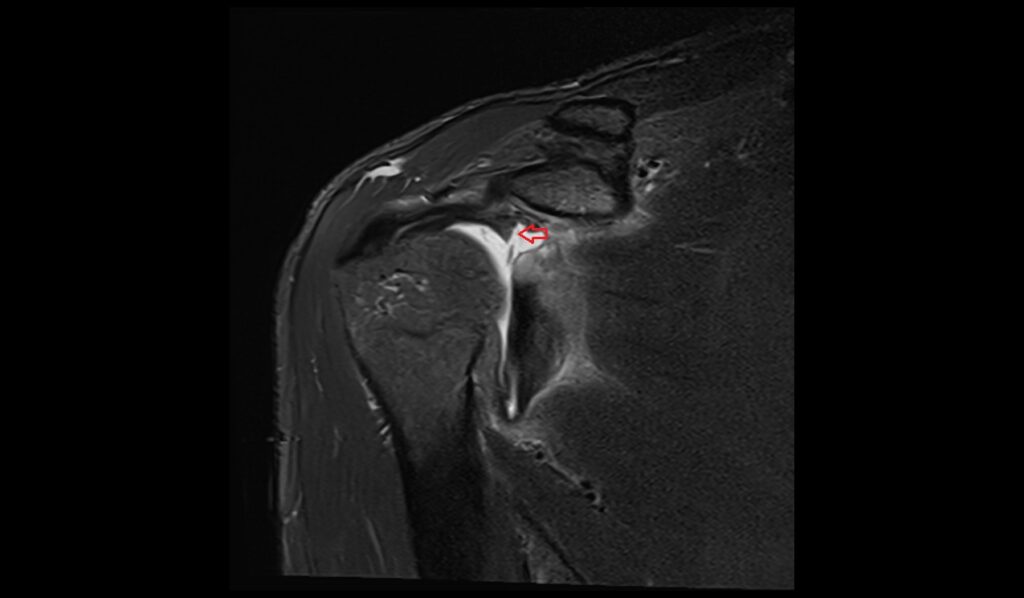
MRI STIR Appearance of ALPSA Lesion
Short Tau Inversion Recovery (STIR) sequences are highly sensitive to fluid and edema, making them ideal for detecting acute injuries and inflammatory changes associated with an ALPSA lesion. On STIR images, the lesion will appear as a hyperintense (bright) area, highlighting the presence of edema and increased water content in the affected tissues. This imaging sequence enhances the visibility of soft tissue abnormalities by suppressing the fat signal, allowing for a clearer assessment of the injury and any associated swelling or fluid accumulation around the labrum and glenoid.
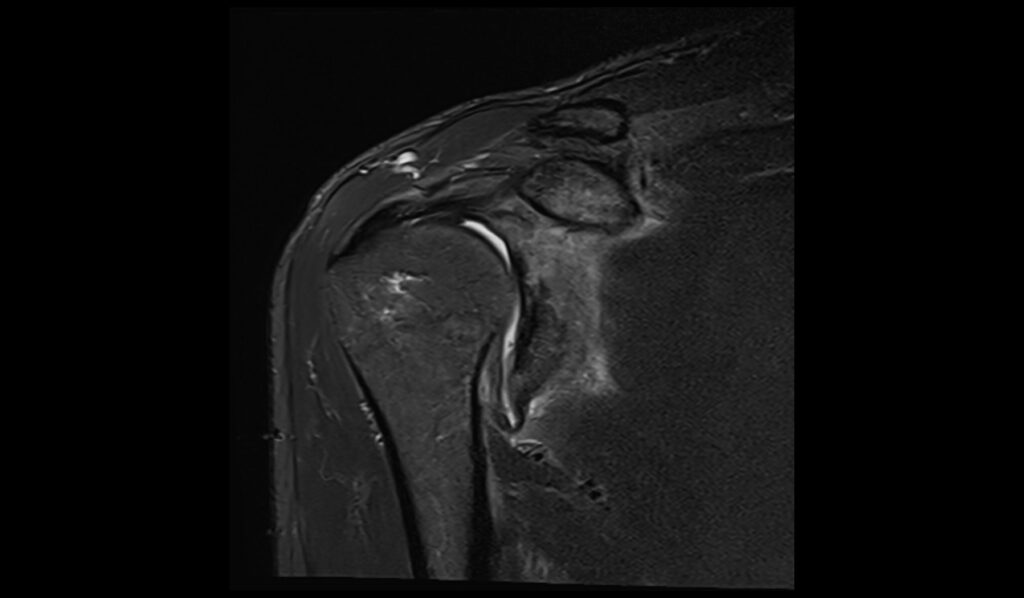
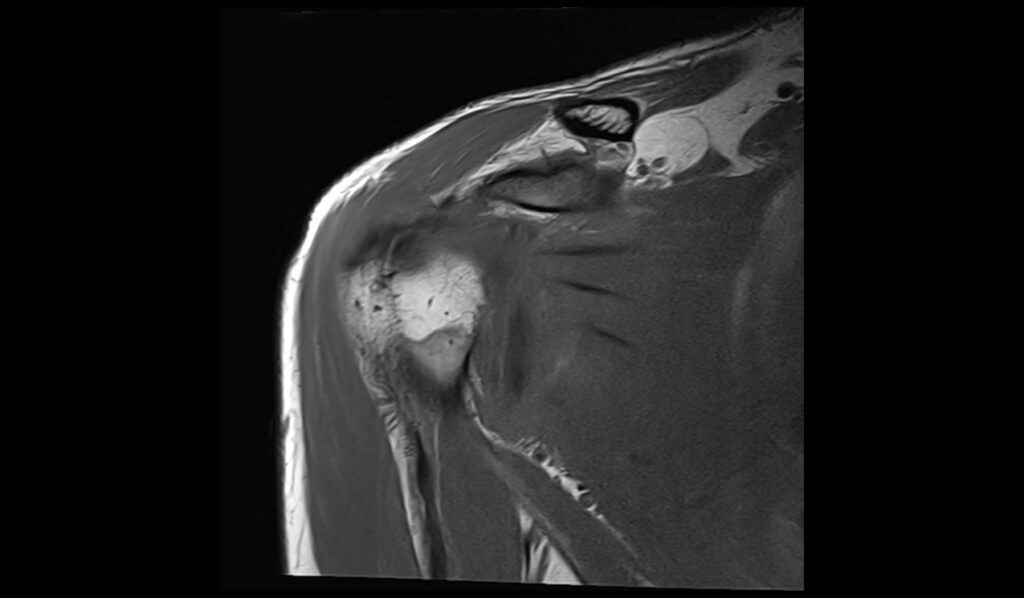
MRI PD Fat-Saturated Appearance of ALPSA Lesion
Proton Density (PD) Fat-Saturated sequences provide detailed images of the soft tissues with high contrast, particularly useful for evaluating the integrity of the labrum and associated structures. On PD fat-saturated images, an ALPSA lesion typically appears as a hyperintense (bright) signal against the suppressed fat background, highlighting the retracted and displaced labral tissue. The PD FS sagittal image is particularly effective in showing the extent of the lesion and the relationship between the labrum and the glenoid. This sequence helps in visualizing the detailed anatomy and any associated capsular or periosteal involvement, making it a crucial tool for comprehensive assessment and diagnosis.
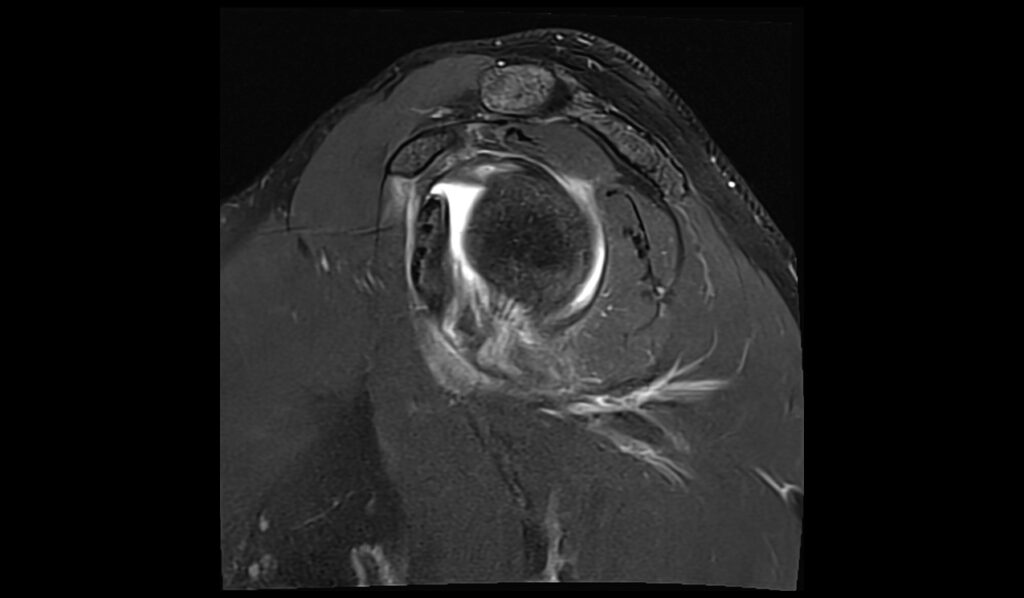
STIR coronal image shows ALPSA Lesion

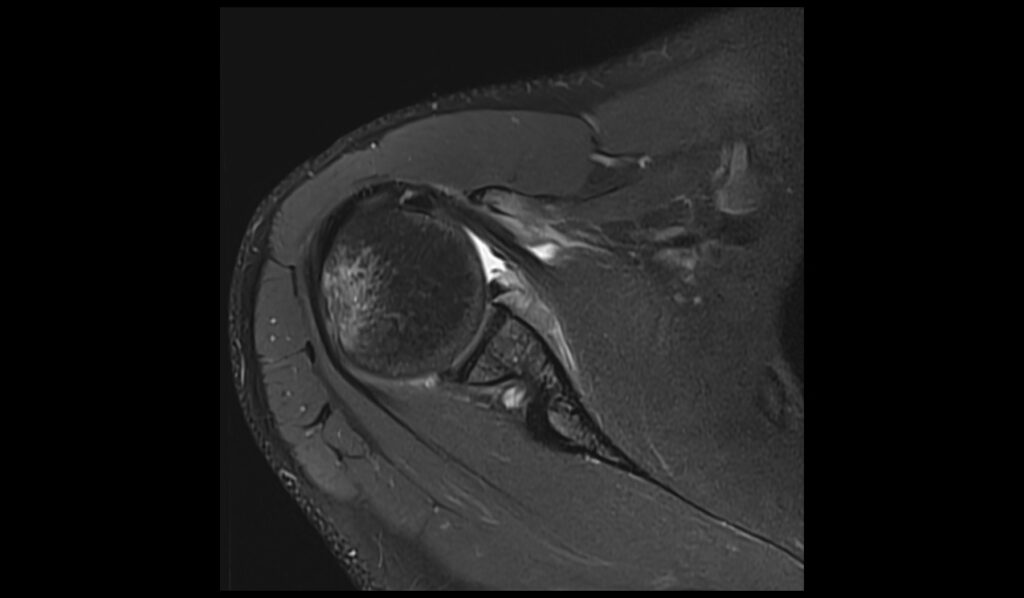
T1 TSE sagittal image shows ALPSA Lesion
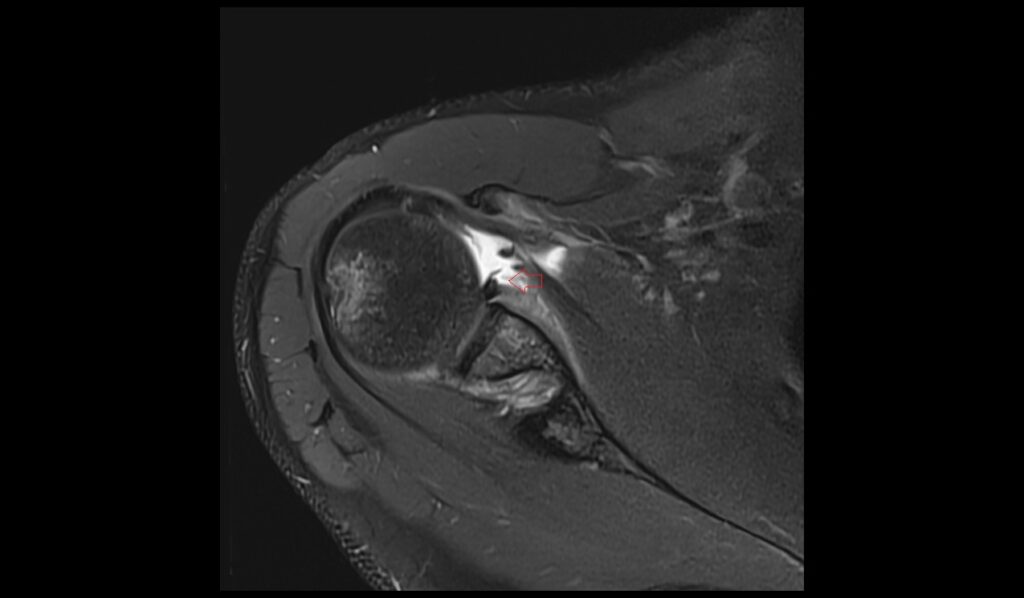
PD FS axial image shows ALPSA Lesion
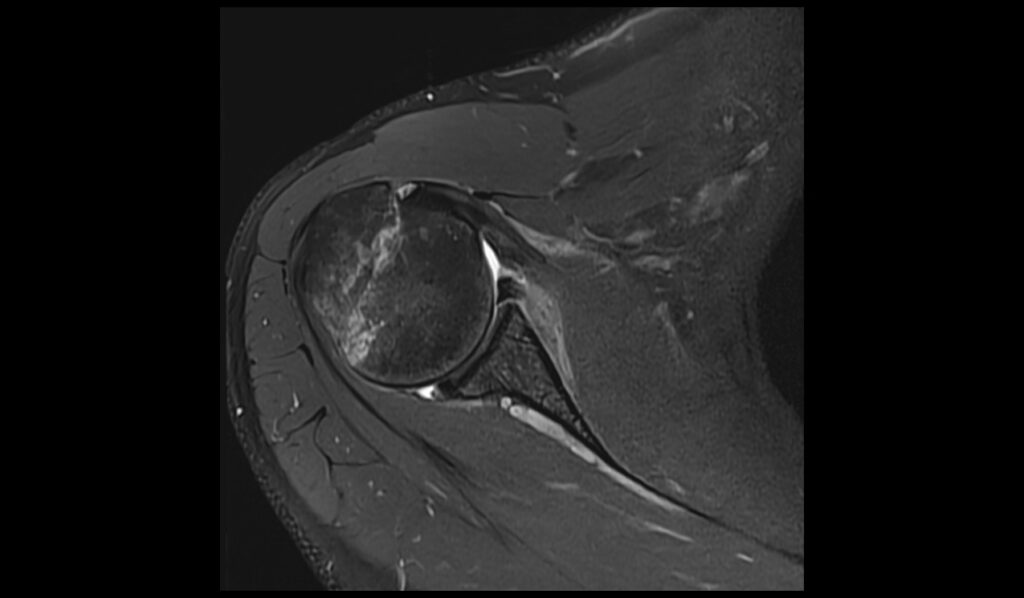
PD FS sagittal image shows ALPSA Lesion


References
- Acid, S., Le Corroller, T., Aswad, R., Pauly, V., & Champsaur, P. (2012). Preoperative imaging of anterior shoulder instability: Diagnostic effectiveness of MDCT arthrography and comparison with MR arthrography and arthroscopy. American Journal of Roentgenology, 198(3), 661-667.
- Bartolomé, A., Pirogova, T., Bartolomé, M.J., Sánchez, R., & García de Lucas, F. (2016). Glenohumeral instability: Validity of low-field MRI for diagnosis of labral tears. Radiology Department, FREMAP MAJADAHONDA Hospital, Madrid, Spain. Available online 26 September 2016.
- Woertler, K., & Waldt, S. (2006). MR imaging in sports-related glenohumeral instability. European Radiology, 16, 2622-2636. https://doi.org/10.1007/s00330-006-0435-4
- Yoon, Y. S., & Cha, J. G. (2023). MRI Findings of Periarticular Lesions with Isolated Greater Tubercle Fractures and Dislocation. Current Medical Imaging, 19(12), 1476-1486. https://doi.org/10.2174/1573405619666230123141247