MRI Anorectal Fistula (Perianal Fistula)
An anorectal fistula, also known simply as a fistula, is an abnormal connection between the epithelialized surface of the anal canal and (usually) the perianal skin. Anorectal fistulas can be painful and can be quite distressing for the person experiencing them.
Causes
Anorectal fistulas often result from an infection in the anal glands that are located in the anus. When these glands get clogged, they can become infected, leading to an abscess. If the abscess doesn’t drain properly, it can extend to the skin surface and create a fistula. However, there can be other causes, such as:
- Crohn’s Disease: Chronic inflammatory disease can affect any part of the gastrointestinal tract and may lead to fistula formation.
- Diverticulitis: Infected diverticula can result in fistulas.
- Injury: Trauma or surgery near the anus may lead to fistula formation.
- Specific Infections: Tuberculosis and sexually transmitted infections may cause fistulas.
- Cancer: Rarely, cancer can cause a fistula to form.
Symptoms
The symptoms of an anorectal fistula can vary depending on its depth and location but often include:
- Pain: Discomfort is often constant and may increase with movement.
- Swelling: There can be swelling around the anus.
- Discharge: There may be a persistent discharge of pus or blood, leading to irritation of the skin around the anus.
- Fecal Leakage: There may be difficulty controlling the bowels.
- Fever: If infection is present, fever and general malaise can occur.
- Recurrent Abscesses: Repeated cycles of infection and healing might be a sign of a fistula.
Treatment
The treatment for anorectal fistulas can depend on their complexity:
Surgery:
- Fistulotomy: The most common treatment, where the fistula tract is cut open and allowed to heal from the inside out.
- Seton Techniques: A seton (a piece of thread or other material) is placed in the fistula to keep it open. This allows it to drain and heal over time.
- Advancement Rectal Flap: A piece of rectal or anal tissue is used to close the internal opening.
- Fibrin Glue Injection: This is a less invasive treatment option where fibrin glue is injected into the fistula to seal the tract.
- Bioprosthetic Plug: A plug that is made of biologically derived material is used to block the internal opening of the fistula.
Medication:
- Antibiotics: These may be prescribed if there’s an infection.
- Immunomodulators: For people with Crohn’s disease, medications that modify the immune response can be helpful.
MRI Appearance of Anorectal Fistula
Magnetic resonance imaging (MRI) is a highly valuable tool in the evaluation of anorectal fistulas. It provides excellent contrast resolution and multiplanar capabilities, allowing for the precise anatomical depiction of the fistulous tract, its relation to the sphincter complex, and any associated abscesses or secondary tracts.
T2-Weighted Images
On T2-weighted images, anorectal fistulas typically appear as hyperintense (bright) linear or curvilinear structures due to the fluid content within the tract. The fistulous tract may be traced from the internal opening within the anal canal to the external opening in the perianal skin. Adjacent inflammatory changes can also be seen, often as hyperintense areas due to edema and inflamed tissue. Any associated abscesses will also appear hyperintense on T2-weighted images because of their fluid content but may show a variable intensity if there’s the presence of debris or granulation tissue.
STIR/T2 Fat-Sat Images
Short Tau Inversion Recovery (STIR) or T2-weighted images with fat saturation are used to suppress the signal from fat, which enhances the visibility of fluid-filled structures like fistulas and abscesses. On STIR/T2 fat-sat images, anorectal fistulas also appear hyperintense, but the contrast between the fistula and the surrounding fat is enhanced because the signal from the fat is suppressed. This makes STIR/T2 fat-sat imaging particularly useful for identifying the presence of small amounts of fluid and differentiating fistulas from surrounding structures.
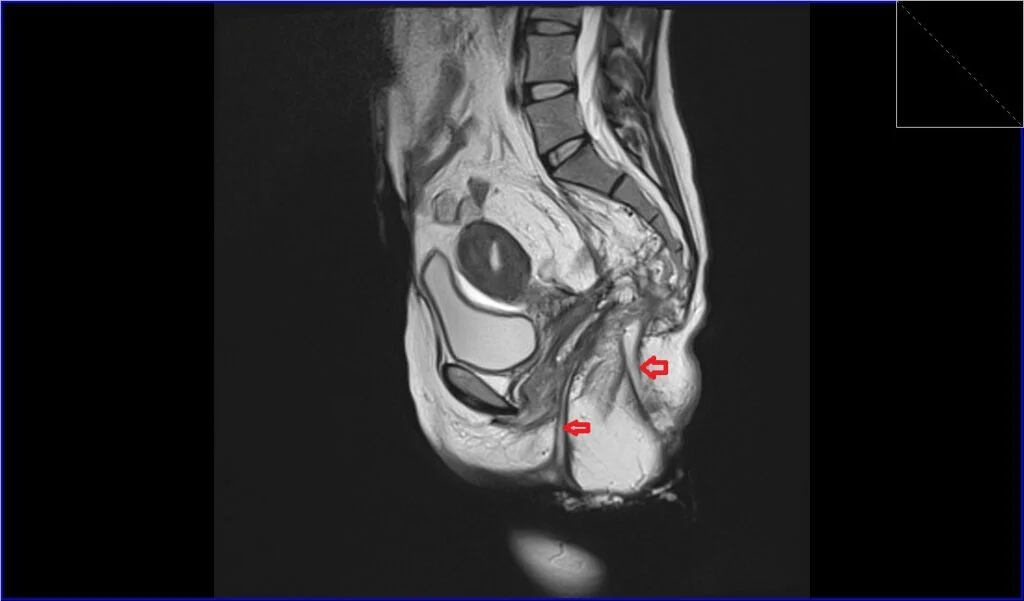
T2 TSE sagittal image shows Anorectal Fistula
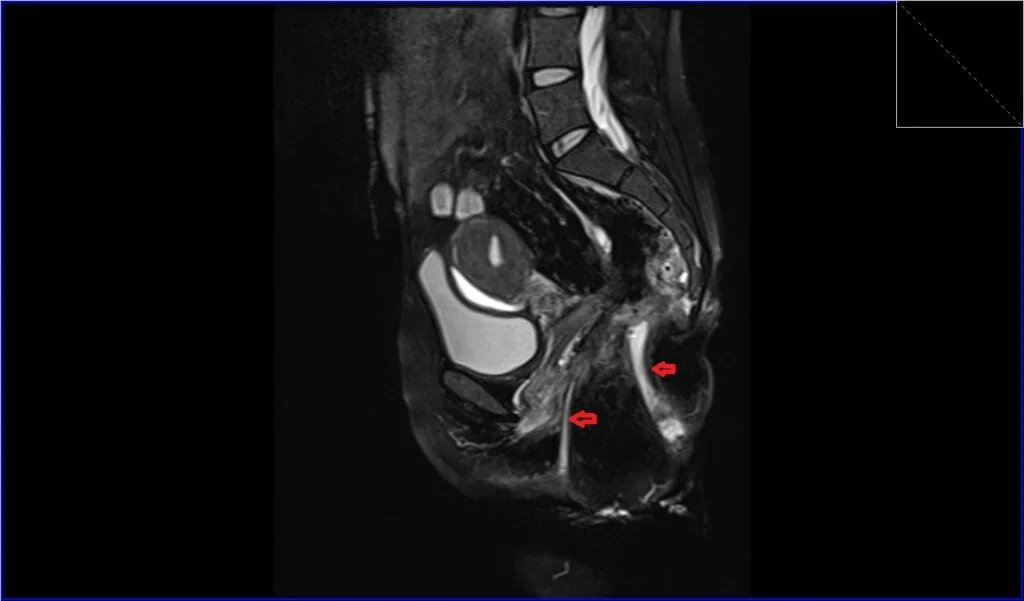
T2 fat saturated sagittal image shows Anorectal Fistula
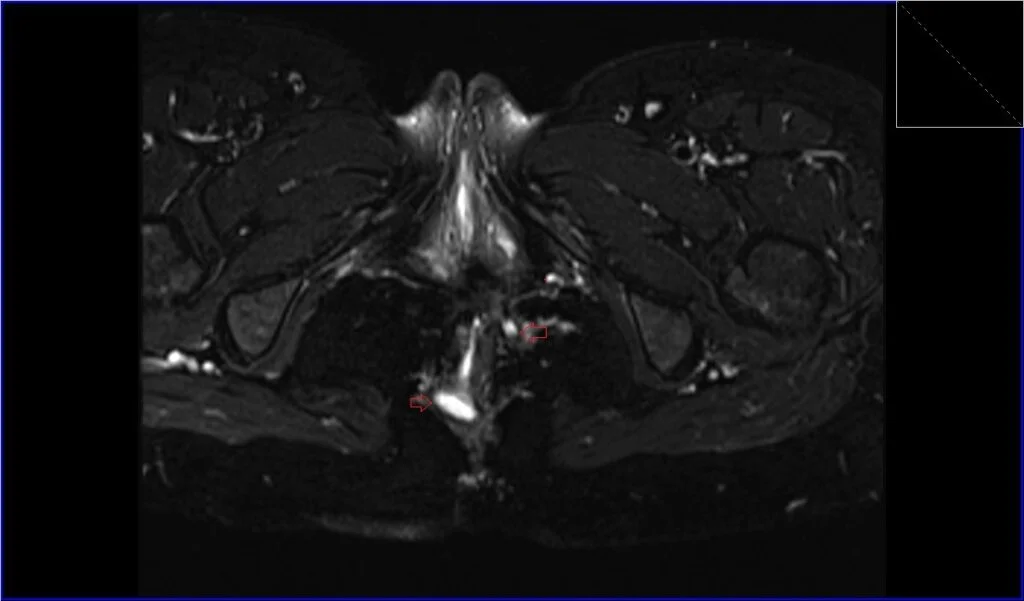
T2 fat saturated axial oblique image shows Anorectal Fistula
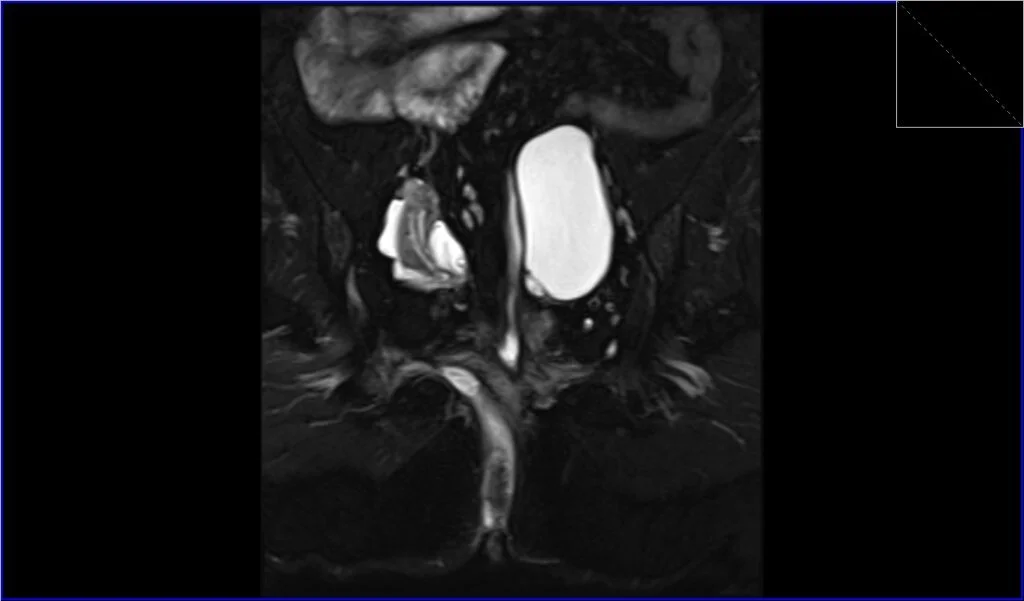
T2 fat saturated coronal oblique image shows Anorectal Fistula
References
- Ramírez Pedraza, N., Pérez Segovia, A. H., Garay Mora, J. A., Techawatanaset, K., Bowman, A. W., Cruz Marmolejo, M. A., Chapa Ibargüengoitia, M., Arizaga Ramírez, S., & Arizaga Ramírez, M. R. (2022). Perianal Fistula and Abscess: An Imaging Guide for Beginners. HomeRadioGraphics, 42(7).
- De Miguel Criado, J., García del Salto, L., Fraga Rivas, P., Aguilera del Hoyo, L. F., Gutiérrez Velasco, L., Díez Pérez de las Vacas, M. I., Marco Sanz, A. G., Manzano Paradela, M., & Fraile Moreno, E. (2011). MR Imaging Evaluation of Perianal Fistulas: Spectrum of Imaging Features. Gastrointestinal Imaging, HomeRadioGraphics, Vol. 32(1). Published online on December 30, 2011. DOI
- Gage, K.L., Deshmukh, S., Macura, K.J., Kamel, I.R., & Zaheer, A. (2013). MRI of Perianal Fistulas: Bridging the radiologic-surgical divide. Abdom Imaging, 38(5), 1033–1042. doi: 10.1007/s00261-012-9965-4
- Liang, C., Lu, Y., Zhao, B., Du, Y., Wang, C., & Jiang, W. (2014). Imaging of Anal Fistulas: Comparison of Computed Tomographic Fistulography and Magnetic Resonance Imaging. Korean Journal of Radiology, 15(6), 712-723.
- Chan CYH, Wong KYK, Kwok SKY, Wong WK, Tang KW. Magnetic Resonance Imaging of Fistula-in-ano. Hong Kong J Radiol. 2015;18:243-52. DOI: 10.12809/hkjr1515300.