Acute pontine infarct MRI
Acute Pontine Infarct
An acute pontine infarct is a type of stroke that occurs in the pons, a part of the brainstem that plays a crucial role in various vital functions such as breathing, sleep, and relaying information between different parts of the brain.
Causes
The primary cause of an acute pontine infarct is the interruption of blood supply to the pons, typically due to:
- Thrombotic or Embolic Occlusion: Blood clots that block blood vessels supplying the pons.
- Atherosclerosis: Narrowing and hardening of the arteries due to the build-up of plaque.
- Hypertension: Chronic high blood pressure can damage blood vessels, leading to strokes.
- Cardiovascular Disease: Conditions such as atrial fibrillation that increase the risk of blood clots.
Symptoms
Symptoms of an acute pontine infarct can vary depending on the exact location and extent of the infarct but often include:
- Weakness or Paralysis: Sudden weakness or paralysis of the face, arms, or legs, usually on one side of the body (hemiparesis).
- Dysarthria: Difficulty speaking or slurred speech.
- Dysphagia: Difficulty swallowing.
- Ataxia: Lack of muscle coordination affecting balance and walking.
- Sensory Disturbances: Numbness or loss of sensation.
- Altered Consciousness: Changes in alertness or consciousness levels.
- Diplopia: Double vision or other visual disturbances.
- Vertigo: A sensation of spinning or loss of balance.
Diagnosis
Diagnosing an acute pontine infarct involves several steps:
- Clinical Examination: Initial assessment of symptoms and medical history.
- Neuroimaging:
- CT Scan: An initial imaging test to rule out hemorrhage and other abnormalities.
- MRI: Magnetic Resonance Imaging is more sensitive for detecting small or early infarcts.
- Blood Tests: To check for risk factors such as high cholesterol, diabetes, and clotting disorders.
- Electrocardiogram (ECG): To detect heart-related issues that could lead to embolic strokes.
- Carotid Ultrasound: To check for blockages in the carotid arteries.
Treatment
Treatment aims to restore blood flow, prevent further strokes, and manage symptoms:
- Thrombolytic Therapy: Administration of clot-busting drugs (e.g., tissue plasminogen activator, tPA) if the patient presents within a specific time window (typically within 4.5 hours of symptom onset).
- Antiplatelet Agents: Medications like aspirin to prevent new clots from forming.
- Anticoagulants: For patients with certain types of embolic strokes, anticoagulants such as warfarin may be prescribed.
- Blood Pressure Management: Controlling high blood pressure through lifestyle changes and medication.
- Statins: To lower cholesterol and stabilize plaque in arteries.
- Rehabilitation: Physical therapy, occupational therapy, and speech therapy to help regain function and adapt to any lasting impairments.
- Supportive Care: Managing symptoms such as swallowing difficulties and providing nutritional support.
MRI appearance of Acute pontine infarct
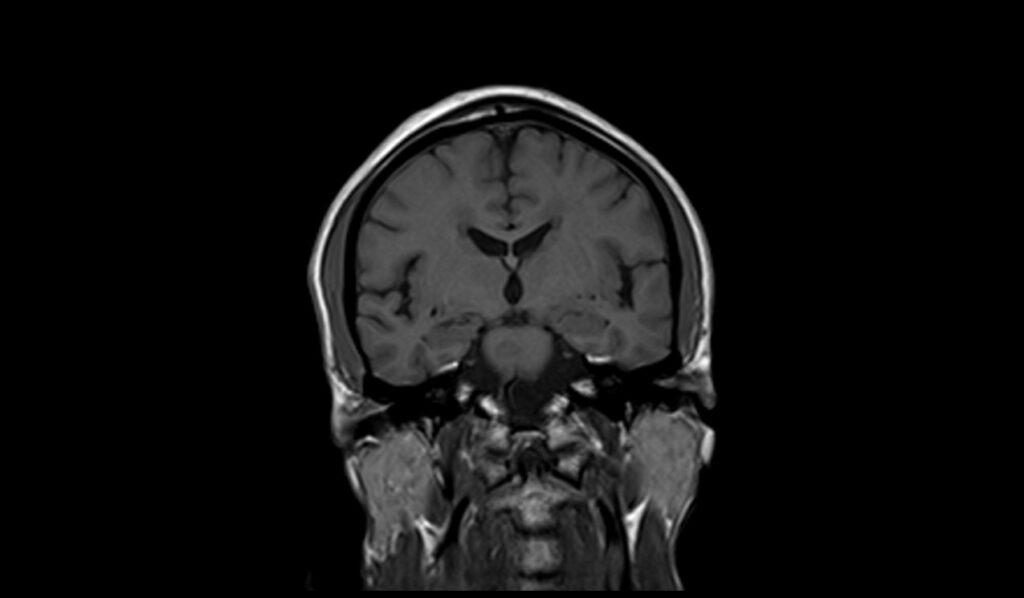
MRI T1 Appearance of Acute Pontine Infarct
On T1-weighted MRI images, an acute pontine infarct typically appears as a hypointense (dark) area within the pons. The reduced signal intensity is due to the loss of normal tissue structure and the presence of edema associated with the infarct. In the early stages of an acute infarct, the changes on T1-weighted images may be subtle, making it less sensitive for early detection compared to other imaging sequences. However, T1 imaging is valuable for anatomical localization and for evaluating the presence of hemorrhage or chronic infarcts.
MRI T2 Appearance of Acute Pontine Infarct
On T2-weighted MRI images, an acute pontine infarct appears as a hyperintense (bright) area within the pons, reflecting the presence of edema and tissue injury. The increased signal intensity on T2 images is due to the higher water content in the affected area. This sequence is particularly useful for identifying the extent of the infarct and the surrounding edema. The bright signal helps in clearly delineating the infarcted region from the normal brain tissue, making T2-weighted imaging a critical component in the assessment of acute pontine infarcts.
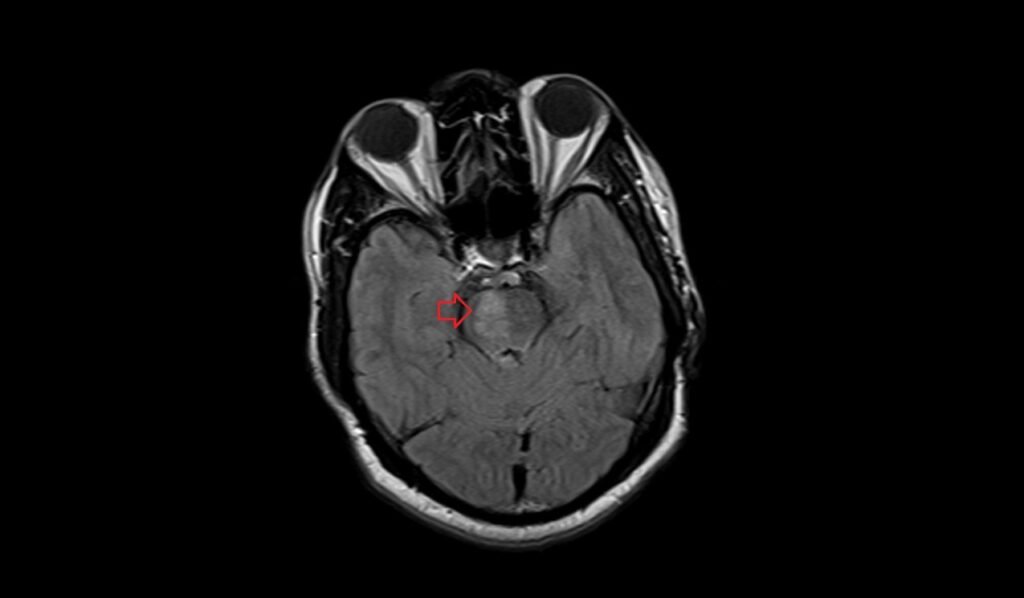
MRI FLAIR Appearance of Acute Pontine Infarct
On FLAIR (Fluid-Attenuated Inversion Recovery) MRI images, an acute pontine infarct presents as a hyperintense (bright) lesion within the pons, similar to T2-weighted images but with the suppression of cerebrospinal fluid (CSF) signal. This suppression of the CSF allows for better contrast between the infarct and the surrounding CSF, enhancing the visibility of the lesion. FLAIR imaging is particularly useful for detecting small infarcts and subtle changes in the brain tissue that might be obscured by the high signal of CSF on standard T2-weighted images.
MRI DWI b0 Appearance of Acute Pontine Infarct
On diffusion-weighted imaging (DWI) with a b-value of 0 (b0), an acute pontine infarct might not be clearly visible, as b0 images primarily show anatomical details similar to T2-weighted images without emphasizing diffusion characteristics. The lesion may appear slightly hyperintense due to T2 shine-through effects, but the true extent and acute nature of the infarct are better evaluated with higher b-values.
MRI DWI b500 Appearance of Acute Pontine Infarct
On DWI with a b-value of 500 (b500), an acute pontine infarct begins to show more prominently as a hyperintense (bright) area within the pons. This increased signal reflects restricted diffusion, a hallmark of acute infarcts due to cytotoxic edema. The higher b-value enhances the sensitivity to diffusion abnormalities, making the infarct more conspicuous compared to the b0 images.
MRI DWI b1000 Appearance of Acute Pontine Infarct
On DWI with a b-value of 1000 (b1000), an acute pontine infarct appears as a markedly hyperintense (bright) lesion, indicating significant restricted diffusion. The high b-value accentuates the diffusion restriction, which is characteristic of acute ischemic stroke. This sequence is highly sensitive for detecting acute infarcts, providing crucial information for early diagnosis and management.
MRI ADC Appearance of Acute Pontine Infarct
On the Apparent Diffusion Coefficient (ADC) map, an acute pontine infarct appears as a hypointense (dark) area, indicating restricted diffusion. The ADC values are derived from DWI sequences and reflect the magnitude of water diffusion within the tissue. In acute infarcts, the cytotoxic edema leads to reduced water mobility, resulting in lower ADC values. This hypointensity on the ADC map confirms the presence of restricted diffusion seen on DWI, distinguishing acute infarcts from other pathologies.
T2 axial images shows Acute pontine infarct

FLAIR axial images shows Acute pontine infarct
T1 coronal images shows Acute pontine infarct
T2 sagittal images shows Acute pontine infarct

DWI b0 images shows Acute pontine infarct

DWI b500 images shows Acute pontine infarct

DWI b1000 images shows Acute pontine infarct

References
- Vlašković, T., Georgievski Brkić, B., Stević, Z., Vukićević, M., Đurović, O., Kostić, D., Stanisavljević, N., Marinković, I., Kapor, S., & Marinković, S. (2022). Anatomic and MRI bases for pontine infarctions with patients presentation. Journal of Stroke and Cerebrovascular Diseases, 31(8), 106613. https://doi.org/10.1016/j.jstrokecerebrovasdis.2022.106613
- Xia, C., Chen, H.-S., Wu, S.-W., & Xu, W.-H. (2017). Etiology of isolated pontine infarctions: A study based on high-resolution MRI and brain small vessel disease scores. BMC Neurology, 17(216). https://doi.org/10.1186/s12883-017-0999-7
- Li, L., Zhu, L., Zeng, J., Liao, S., Zhang, S., Yu, J., & Yang, Z. (2009). Pontine infarction with pure motor hemiparesis or hemiplegia: A prospective study. BMC Neurology, 9(25). https://doi.org/10.1186/1471-2377-9-25
- González, R. G. (2012). Clinical MRI of Acute Ischemic Stroke. Journal of Magnetic Resonance Imaging, 36(2), 259–271. https://doi.org/10.1002/jmri.23595. PMCID: PMC3400122. PMID: 22807220.